Assessment |
Biopsychology |
Comparative |
Cognitive |
Developmental |
Language |
Individual differences |
Personality |
Philosophy |
Social |
Methods |
Statistics |
Clinical |
Educational |
Industrial |
Professional items |
World psychology |
Biological: Behavioural genetics · Evolutionary psychology · Neuroanatomy · Neurochemistry · Neuroendocrinology · Neuroscience · Psychoneuroimmunology · Physiological Psychology · Psychopharmacology (Index, Outline)
Sleeping Princess: A 1926 painting by Victor Vasnetsov
The neuroscience of sleep is the study of the neuroscientific and physiological basis of the nature of sleep and its functions. Traditionally, sleep has been studied as part of psychology and medicine.[1] The study of sleep from a neuroscience perspective grew to prominence with advances in technology and proliferation of neuroscience research from the second half of the twentieth century.
The fact that organisms spend about a third of their time in sleep, and that sleep deprivation can have disastrous effects ultimately leading to death[2][3] demonstrate the importance of sleep. For a phenomenon so important, the purposes and mechanisms of sleep are only partially understood, so much that it has been quipped "The only known function of sleep is to cure sleepiness".[How to reference and link to summary or text] However, the development of improved imaging techniques like EEG, PET and fMRI, along with high computational power have led to an increasingly greater understanding of the mechanisms underlying sleep.
The fundamental questions in the neuroscientific study of sleep are - 1) What are the correlates of sleep i.e. what are the minimal set of events that could confirm that the organism is sleeping? 2) How is sleep triggered and regulated by the brain and the nervous system? 3) What happens in the brain during sleep? 4) How can we understand sleep function based on physiological changes in the brain? 5) What causes various sleep disorders and how can they be treated?[4]
Other areas of modern neuroscience sleep research include the evolution of sleep, sleep during development and aging, animal sleep, mechanism of effects of drugs on sleep, dreams and nightmares, and stages of arousal between sleep and wakefulness.[5]
Introduction[]
- Main article: Sleep
Sleep is a naturally recurring state characterized by reduced or absent consciousness, relatively suspended sensory activity, and inactivity of nearly all voluntary muscles. In mammals and birds, sleep is broadly divided into two types- rapid eye movement (REM) and non-rapid eye movement (NREM or non-REM) sleep. NREM sleep itself is divided into multiple stages- N1, N2 and N3. Sleep proceeds in cycles of REM and NREM, the order normally being N1 → N2 → N3 → N2 → REM. Of the two, NREM is considered to be deep sleep (the deepest part of NREM is called slow wave sleep), and is characterized by lack of prominent eye movement or muscle paralysis. On the other hand, REM sleep is considered closer to wakefulness and is characterized by rapid eye movement and muscle atonia. It is during REM sleep that dreams (or nightmares) occur.
Sleep timing is controlled by the circadian clock, and in humans, to some extent by willed behavior. The term circadian comes from the Latin circa, meaning "around" (or "approximately"), and diem or dies, meaning "day". The circadian clock refers to a biological mechanism that governs multiple biological processes causing them to display an endogenous, entrainable oscillation of about 24 hours. These rhythms have been widely observed in plants, animals, fungi and cyanobacteria.
Sleep is considered an essential function for animals, though it is not yet sure why this is so. However, sleep deprivation can lead to drastic consequences, and inadequate sleep can lead to sleep debt. Also, sleep at any time of the day is not equivalent and it is most effective only when it coincides with certain biological processes.
Correlates of sleep[]
One of the important questions in sleep research is clearly defining the sleep state. This problem arises because sleep was traditionally defined as a state of consciousness and not as a physiological state,[6][7] thus there was no clear definition of what minimum set of events constitute sleep and distinguish it from other states of partial or no consciousness. The problem of making such a definition is complicated because it needs to include a variety of modes of sleep found across different species.
At a symptomatic level, sleep is characterized by lack of reactivity to sensory inputs, low motor output, diminished conscious awareness and rapid reversibility to wakefulness.[8] However, to translate these into a biological definition is difficult because no single pathway in the brain is responsible for the generation and regulation of sleep. One of the earliest proposals was to define sleep as the deactivation of the cerebral cortex and the thalamus[9] because of near lack of response to sensory inputs during sleep. However, this was invalidated because both regions are active in some phases of sleep. In fact, it appears that the thalamus is only deactivated in the sense of transmitting sensory information to the cortex.[10]
Some of the other observations about sleep included decrease of sympathetic activity and increase of parasympathetic activity in non-REM sleep, and increase of heart rate and blood pressure accompanied by decrease in homeostatic response and muscle tone during REM sleep.[11][12] However, these symptoms are not limited to sleep situations and do not map to specific physiological definitions.
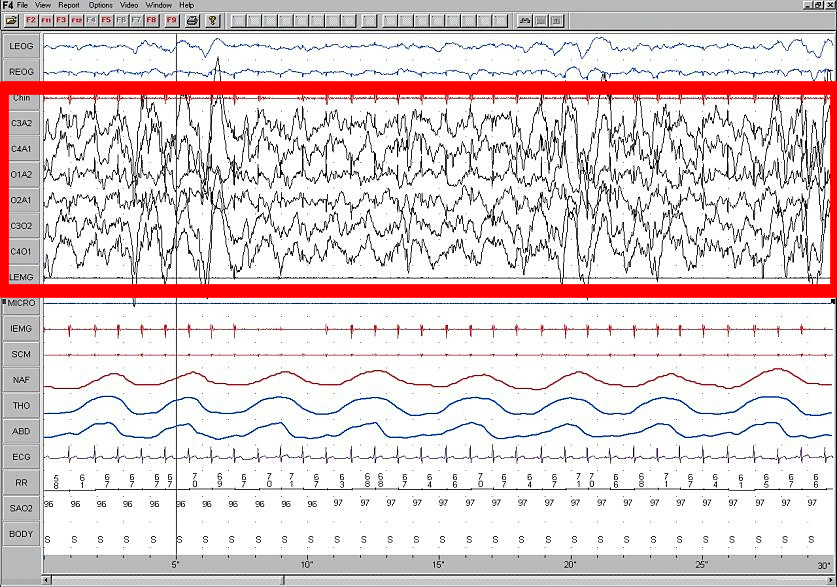
More recently, the problem of definition has been addressed by observing overall brain activity in the form of characteristic EEG patterns.[13] Each stage of sleep and wakefulness has a characteristic pattern of EEG which can be used to identify the stage of sleep. Waking is usually characterized by beta (12–30 Hz) and gamma (25–100 Hz) depending on whether there was a peaceful or stressful activity.[14] The onset of sleep involves slowing down of this frequency to the drowsiness of alpha (8–12 Hz) and finally to theta (4–10 Hz) of Stage 1 NREM sleep.[15] This frequency further decreases progressively through the higher stages of NREM and REM sleep. On the other hand, the amplitude of sleep waves is lowest during wakefulness (10-30μV) and shows a progressive increase through the various stages of sleep. Stage 2 is characterized by sleep spindles (intermittent clusters of waves at sigma frequency i.e. 12–14 Hz) and K complexes (sharp upward deflection followed by slower downward deflection). Stage 3 sleep has more sleep spindles.[16][17][18] Stages 3 and 4 have very high amplitude delta waves (0–4 Hz) and are known as slow wave sleep.[19] REM sleep is characterized by low amplitude, mixed frequency waves- a sawtooth wave pattern is often present.[20]
Ontogeny and phylogeny of sleep[]
Animal Sleep: Image of a sleeping white tiger
The questions of how sleep evolved in the animal kingdom and how it developed in humans are especially important because they might provide a clue to the functions and mechanisms of sleep respectively.
Sleep evolution[]
Sleep (especially deep SWS and REM) is tricky behavior because it steeply increases predation risk. This means that, for sleep to have evolved, the functions of sleep should have provided a substantial advantage over the risk it entails. In fact, studying sleep in different organisms shows how they have balanced this risk by evolving partial sleep mechanisms or by having protective habitats. Thus, studying the evolution of sleep might give a clue not only to the developmental aspects and mechanisms, but also to an adaptive justification for sleep.
One challenge studying sleep evolution is that adequate sleep information is known only for two classes of animals- chordata and arthropoda.[5] With the available data, comparative studies have been used to determine how sleep might have evolved. One question that scientists try to answer through these studies is whether sleep evolved only once or multiple times. To understand this, they look at sleep patterns in different classes of animals whose evolutionary histories are fairly well-known and study their similarities and differences.
Humans possess both slow wave and REM sleep, in both phases both eyes are closed and both hemispheres of the brain involved. Sleep has also been recorded in mammals other than humans. One interesting study showed that echidnas possess only slow wave sleep (non-REM). This seems to indicate that REM sleep appeared in evolution only after therians.[21] But this has later been contested by studies that claim that sleep in echidna combines both modes into a single sleeping state.[22] Other studies have shown a peculiar form of sleep in odontocetes (like dolphins and porpoises). This is called the unihemispherical slow wave sleep (USWS). At any time during this sleep mode, the EEG of one brain hemisphere indicates sleep while that of the other is equivalent to wakefulness. In some cases, the corresponding eye is open. This might allow the animal to reduce predator risk and sleep while swimming in water, though the animal may also be capable of sleeping at rest.[23][24]
The correlates of sleep found for mammals are valid for birds as well i.e. bird sleep is very similar to mammals and involves both SWS and REM sleep with similar features, including closure of both eyes, lowered muscle tone,etc.[25] However, the proportion of REM sleep in birds is much lower. Also, some birds can sleep with one eye open if there is high predation risk in the environment.[26][27] This gives rise to the possibility of sleep in flight; considering that sleep is very important and some bird species can fly for weeks continuously, this seems to be the obvious result. However, sleep in flight has not been recorded, and is so far unsupported by EEG data. Further research may explain whether birds sleep during flight or if there are other mechanisms which ensure their remaining healthy during long flights in the absence of sleep.
Unlike in birds, very few consistent features of sleep have been found among reptile species. The only common observation is that reptiles do not have REM sleep.[5]
Sleep in some invertebrates has also been extensively studied, for e.g., sleep in fruitflies (Drosophila)[28] and honeybees.[29] Some of the mechanisms of sleep in these animals have been discovered while others remain quite obscure. The features defining sleep have been identified for the most part, and like mammals, this includes reduced reaction to sensory input, lack of motor response in the form of antennal immobility, etc.
The fact that both the forms of sleep are found in mammals and birds, but not in reptiles (which are considered to be an intermediate stage) indicates that sleep might have evolved separately in both. Substantiating this might be followed by further research on whether the EEG correlates of sleep are involved in its functions or if they are merely a feature. This might further help in understanding the role of sleep in long term plasticity.
Sleep development and aging[]
The ontogeny of sleep is the study of sleep across different age groups of a species, particularly during development and aging. Among mammals, infants sleep the longest.[30] Human babies have 8 hours of REM sleep and 8 hours of NREM sleep on an average. The percentage of time spent on each mode of sleep varies greatly in the first few weeks of development and some studies have correlated this to the degree of precociality of the child.[31] Within a few months of postnatal development, there is a marked reduction in percentage of hours spent in REM sleep. By the time the child becomes an adult, he spends about 6–7 hours in NREM sleep and only about an hour in REM sleep.[32][33] This is true not only of humans, but of many animals dependent on their parents for food.[34] The observation that the percentage of REM sleep is very high in the first stages of development has led to the hypothesis that REM sleep might facilitate early brain development.[31] However, this theory has been contested by other studies.
Sleep behavior undergoes substantial changes during adolescence- some of these changes may be societal in humans, but other changes are hormonal. Another important change is the decrease in the number of hours of sleep, as compared to childhood, which gradually becomes identical to an adult. It is also being speculated that homeostatic regulation mechanisms may be altered during adolescence. Apart from this, the effect of changing routines of adolescents on other behavior such as cognition and attention is yet to be studied.[35][36]
Sleep in aging is another equally important area of research. A common observation is that many older adults spend time awake in bed after sleep onset in an inability to fall asleep and experience marked decrease in sleep efficiency.[37] There may also be some changes in circadian rhythms.[38] Studies are ongoing about what causes these changes and how they maybe reduced to ensure comfortable sleep of old adults.
Brain activity during sleep[]
{kind=link}
{kind=link}
{kind=link}
Understanding the activity of different parts of the brain during sleep can give a clue to the functions of sleep. It has been observed that mental activity is present during all stages of sleep, though from different regions in the brain. So, contrary to popular understanding, the brain never completely shuts down. Also, sleep intensity of a particular region is homeostatically related to the corresponding amount of activity before sleeping.[39][40] The use of imaging modalities like PET and fMRI, combined with EEG recordings, gives a clue to which brain regions participate in creating the characteristic wave signals and what their functions might be.
NREM sleep activity[]
NREM sleep is characterized by decreased global and regional cerebral blood flow. Initially, it was expected that the brainstem, which was implicated in arousal would be inactive, but this was later on found to have been due to low resolution of PET studies and it was shown that there is some slow wave activity in the brainstem as well. However, other parts of the brain, including the precuneus, basal forebrain and basal ganglia are deactivated during sleep. Many areas of the cortex are also inactive, but to different levels. For example, the ventromedial prefrontal cortex is considered the least active area while the primary cortex, the least deactivated.[17][41]
NREM sleep is characterized by slow oscillations, spindles and delta waves. The slow oscillations have been shown to be from the cortex, as lesions in other parts of the brain do not affect them, but lesions in the cortex do.[42] The delta waves have been shown to be generated by reciprocally connected thalamic and cortical neural circuits. During sleep, the thalamus stops relaying sensory information to the brain, however it continues to produce signals that are sent to its cortical projections. These waves are generated in the thalamus even in the absence of the cortex, but the cortical output seems to play a role in the simultaneous firing by large groups of neurons.[43] The thalamic reticular nucleus is considered to be the pacemaker of the sleep spindles. This has been further substantiated by the fact that rhythmic stimulation of the thalamus leads to increased secondary depolarization in cortical neurons, which further results in the increased amplitude of firing, causing self-sustained activity. The sleep spindles have been predicted to play a role in disconnecting the cortex from sensory input and allowing entry of calcium ions into cells, thus potentially playing a role in Plasticity.[44][45]
REM sleep activity[]
REM sleep is characterized by high global cerebral blood flow, comparable to wakefulness.[46] In fact, many areas in the cortex have been recorded to have more blood flow during REM sleep than even wakefulness- this includes the hippocampus, temporal-occipital areas, some parts of the cortex, and basal forebrain. The limbic and paralimbic system including the amygdala are other active regions during REM sleep.[46][47] Though the brain activity during REM sleep appears very similar to wakefulness, the main difference between REM and wakefulness is that, arousal in REM is more effectively inhibited. This, along with the virtual silence of monoaminergic neurons in the brain, maybe said to characterize REM.[48]
In EEG recordings, REM sleep is characterized by high frequency, low amplitude activity and spontaneous occurrence of beta and gamma waves. The best candidates for generation of these fast frequency waves are fast rhythmic bursting neurons in corticothalamic circuits. Unlike in slow wave sleep, the fast frequency rhythms are synchronized over restricted areas in specific local circuits between thalamocortical and neocortical areas. These are said to be generated by cholinergic processes from brainstem structures.
Apart from this, the amygdala plays a role in REM sleep modulation, supporting the hypothesis that REM sleep allows internal information processing. The high amygdalar activity may also cause the emotional responses during dreams.[49] Similarly, the bizarreness of dreams may be due to the decreased activity of prefrontal regions, which are involved in integrating information as well as episodic memory.
Ponto-geniculo-occipital waves[]
REM sleep is also related to the firing of ponto-geniculo-occipital waves (also called phasic activity or PGO waves) and activity in the cholinergic ascending arousal system. The PGO waves have been recorded in the lateral geniculate nucleus and occipital cortex during the pre-REM period and are thought to represent dream content. The greater signal-to-noise ratio in the LG cortical channel suggests that visual imagery in dreams may appear before full development of REM sleep, but this has not yet been confirmed. PGO waves may also play a role in development and structural maturation of brain, as well as long term potentiation in immature animals, based on the fact that there is high PGO activity during sleep in the developmental brain.[50][51]
Network reactivation[]
The other form of activity during sleep is reactivation- some electrophysiological studies have shown that neuronal activity patterns found during a learning task before sleep are reactivated in the brain during sleep.[52] This, along with the coincidence of active areas with areas responsible for memory have led to the theory that sleep might have some memory consolidation functions. In this relation, some studies have shown that after a sequential motor task, the pre-motor and visual cortex areas involved are most active during REM sleep, but not during NREM. Similarly, the hippocampal areas involved in spatial learning tasks are reactivated in NREM sleep, but not in REM. Such studies suggest a role of sleep in consolidation of specific memory types. It is, however, still unclear whether other types of memory are also consolidated by these mechanisms.[53]
Hippocampal neocortical dialog[]
The hippocampal neocortical dialog refers to the very structured interactions during SWS between groups of neurons called ensembles in the hippocampus and neocortex.[54][55] Sharp wave patterns (SPW) dominate the hippocampus during SWS and neuron populations in the hippocampus participate in organized bursts during this phase. This is done in synchrony with state changes in the cortex (DOWN/UP state) and coordinated by the slow oscillations in cortex. These observations, coupled with the knowledge that the hippocampus plays a role in short to medium term memory whereas the cortex plays a role in long term memory, have led to the hypothesis that the hippocampal neocortical dialog might be a mechanism through which the hippocampus transfers information to the cortex. Thus, the hippocampal neocortical dialog is said to play a role in memory consolidation.[56]
Sleep regulation[]
Sleep regulation refers to the control of when an organism transitions between sleep and wakefulness.[57] The key questions here are to identify which parts of the brain are involved in sleep onset and what their mechanisms of action are.[58] In humans and most animals sleep and wakefulness seems to follow an electronic flip-flop model i.e. both states are stable, but the intermediate states are not.[59][60] Of course, unlike in the flip-flop, in the case of sleep, there seems to be a timer ticking away from the minute of waking so that after a certain period one must sleep, and in such a case even waking becomes an unstable state. The reverse may also be true to a lesser extent.
Sleep onset[]
Some light was thrown on the mechanisms on sleep onset by the discovery that lesions in the preoptic area and anterior hypothalamus lead to insomnia while those in the posterior hypothalamus lead to sleepiness.[61][62] Apart from this, it was found that lesions in oral pontine and midbrain reticular formation lead to loss of cortical activation.[63] This was further narrowed down to show that the central midbrain tegmentum is the region that plays a role in cortical activation. Thus, sleep onset seems to arise from activation of the anterior hypothalamus along with inhibition of the posterior regions and the central midbrain tegmentum. Further research has shown that the hypothalamic region called ventrolateral preoptic nucleus produces the inhibitory neurotransmitter GABA that inhibits the arousal system during sleep onset.[59]
Models of sleep regulation[]
Sleep is regulated by two parallel mechanisms- homeostatic regulation and circadian regulation, controlled by the hypothalamus and the suprachiasmatic nucleus (SCN) respectively. Although the exact nature of sleep drive is unknown, homeostatic pressure builds up during wakefulness and this continues until the person goes to sleep. Adenosine is thought to play a critical role in this and many people have proposed that the pressure build-up is partially due to adenosine accumulation. However, some researchers have shown that accumulation alone does not explain this phenomenon completely. The circadian rhythm is a 24 hr cycle in the body, which has been shown to continue even in the absence of environmental cues. This is caused by projections from the SCN to the brain stem.
This two process model was first proposed in 1982 by Borbely,[64] who called them Process S (homeostatic) and Process C (Circadian) respectively. He showed how the slow wave density increases through the night and then drops off at the beginning of the day while the circadian rhythm is like a sinusoid. He proposed that the pressure to sleep was the maximum when the difference between the two was highest.
In 1993, a different model called the opponent process model[65] was proposed. This model explained that these two processes opposed each other to produce sleep, as against Borbely's model. According to this model, the SCN, which is involved in the circadian rhythm, enhances wakefulness and opposes the homeostatic rhythm. In opposition is the homeostatic rhythm, regulated via a complex multisynaptic pathway in the hypothalamus that acts like a switch and shuts off the arousal system. Both effects together produce a see-saw like effect of sleep and wakefulness.[48]
More recently, it has been proposed that both models have some validity to them, while new theories hold that inhibition of NREM sleep by REM could also play a role.[66] In any case, the two process mechanism adds flexibility to the simple circadian rhythm and could have evolved as an adaptive measure.
Thalamic regulation[]
Much of the brain activity in sleep has been attributed to the thalamus and it appears that the thalamus may play a critical role in SWS. The two primary oscillations in slow wave sleep- delta and the slow oscillation can be generated by both the thalamus and the cortex. However, sleep spindles can only be generated by the thalamus, making its role very important. The thalamic pacemaker hypothesis[67] holds that these oscillations are generated by the thalamus but the synchronization of several groups of thalamic neurons firing simultaneously depends on the thalamic interaction with the cortex. The thalamus also plays a critical role in sleep onset when it changes from tonic to phasic mode, thus acting like a mirror for both central and decentral elements and linking distant parts of the cortex to co-ordinate their activity.[68][69][70]
Reticular activating system[]
The reticular activating system consists of three groups of neurons in the brain stem- pedunculopontine nucleus, locus caeruleus and raphe nucleus.[71] When awake, it receives all kinds of non-specific sensory information and relays them to the cortex. It also modulates fight or flight responses and is hence linked to the motor system. During sleep onset, it acts via two pathways- the first is the cholinergic pathway[72] that clears the way for thalamocortical transmission; the second is the monoaminergic pathway (which starts in the upper brain and projects to the hypothalamus and cerebral cortex) that can cause wakefulness if inactive.[59] It is also predicted to play a role in REM sleep by modulating muscle tone, causing the muscle atonia characteristic of REM sleep. During NREM sleep this system is blocked by the preoptic nucleus neurons.
Sleep function[]
The need and function of sleep are among the least clearly understood areas in sleep research. While some functions of sleep are known, others have been proposed but not completely substantiated or understood. Some of the early ideas about sleep function were based on the fact that most (if not all) external activity is stopped during sleep. Initially, it was thought that sleep was simply a mechanism for the body to "take a break" and reduce wear. Later observations of the low metabolic rates in the brain during sleep seemed to indicate some metabolic functions of sleep.[73] With the development of EEG, it was found that the brain has almost continuous internal activity during sleep, leading to the idea that the function could be that of reorganization or specification of neuronal circuits or strengthening of connections.[74][75] These hypotheses are still being explored. Other proposed functions of sleep include- maintaining hormonal balance, temperature regulation and maintaining heart rate.
Endocrine function[]
The secretion of many hormones is affected by sleep-wake cycles. For example, melatonin, a hormonal timekeeper, is considered a strongly circadian hormone, whose secretion increases at dim light and peaks during nocturnal sleep, diminishing with bright light to the eyes.[76] In some organisms melatonin secretion depends on sleep, but in humans it is independent of sleep and depends only on light level. Of course, in humans as well as other animals, such a hormone may facilitate coordination of sleep onset. Similarly, cortisol and thyroid stimulating hormone (TSH) are strongly circadian and diurnal hormones, mostly independent of sleep.[77] In contrast, other hormones like growth hormone (GH) & prolactin are critically sleep-dependent, and are suppressed in the absence of sleep.[78] GH has maximum increase during SWS while prolactin is secreted early after sleep onset and rises through the night. In some hormones whose secretion is controlled by light level, sleep seems to increase secretion. Almost in all cases, sleep deprivation has detrimental effects. For example, cortisol, which is essential for metabolism (it is so important that animals can die within a week of its deficiency) and affects the ability to withstand noxious stimuli, is increased by waking and during REM sleep.[79] Similarly, TSH increases during nocturnal sleep and decreases with prolonged periods of reduced sleep, but interestingly, increases during total acute sleep deprivation.[80][81]
Because hormones play a major role in energy balance and metabolism, and sleep plays a critical role in the timing and amplitude of their secretion, sleep has a sizable effect on metabolism. This could explain some of the early theories of sleep function that predicted that sleep has a metabolic regulation role.
Memory processing[]
- Main article: Sleep and Memory
The role of sleep in memory has long been suspected. Many initial studies focused primarily on testing the effect of sleep on memory after training a particular task (posttraining), but later studies have also confirmed the importance of pretraining sleep on learning a new task. Such behavioral and imaging measures in tests with both animal and human subjects have shown that pretraining sleep plays a critical role in preparing the memory for encoding and posttraining sleep plays a major role in memory consolidation.
Further studies have looked at the specific effects of different stages of sleep on different types of memory. For example, it has been found that sleep deprivation does not significantly affect recognition of faces, but can produce a significant impairment of temporal memory (discriminating which face belonged to which set shown). Sleep deprivation was also found to increase beliefs of being correct, especially if they were wrong. Another study reported that the performance on free recall of a list of nouns is significantly worse when sleep deprived (an average of 2.8 ± 2 words) compared to having a normal night of sleep (4.7 ± 4 words). These results indicate the role of sleep on declarative memory formation. This has been further confirmed by observations of low metabolic activity in the prefrontal cortex and temporal and parietal lobes for the temporal learning and verbal learning tasks respectively. Data analysis has also shown that the neural assemblies during SWS correlated significantly more with templates than during waking hours or REM sleep. Also, post-learning, post-SWS reverberations lasted 48 hours, much longer than the duration of novel object learning (1 hour), indicating long term potentiation.
Other interesting observations include the importance of napping- improved performance in some kinds of tasks after a 1 hour afternoon nap; studies of performance of shift workers- showing that an equal number of hours of sleep in the day is not the same as in the night. Current research studies look at the molecular and physiological basis of memory consolidation during sleep. These, along with studies of genes that may play a role in this phenomenon, together promise to give a more complete picture of the role of sleep in memory.
Sleep can also serve to weaken synaptic connections that were acquired over the course of the day but which are not essential to optimal functioning. In doing so, the resource demands can be lessened, since the upkeep and strengthening of synaptic connections constitutes a large portion of energy consumption by the brain and tax other cellular mechanisms such as protein synthesis for new channels. [82] Without a mechanism like this taking place during sleep, the metabolic needs of the brain would increase over repeated exposure to daily synaptic strengthening, up to a point where the strains become excessive or untenable.
Behavior change with sleep deprivation[]
Sleep deprivation is common and sometimes even necessary in modern societies because of occupational and domestic reasons like round-the-clock service, security or media coverage, cross-time-zone projects etc. This makes understanding the effects of sleep deprivation very important. Though many studies have been done from the early 1900s to document the effect of sleep deprivation, the neurobehavioral basis for these has been studied only recently.
Sleep deprivation has been strongly correlated with increased probability of accidents and industrial errors.[83][84] Many studies have shown the slowing of metabolic activity in the brain with many hours of sleep debt.[80] Some studies have also shown that the attention network in the brain is particularly affected by lack of sleep,[85] and though some of the effects on attention may be masked by alternate activities (like standing or walking) or caffeine consumption,[86] attention deficit cannot be completely avoided.
Sleep deprivation has been shown to have a detrimental effect on cognitive tasks, especially involving divergent functions or multitasking.[83][87][88] It also has effects on mood and emotion, and there have been multiple reports of increased tendency for rage, fear or depression with sleep debt.[89][90] However, some of the higher cognitive functions seem to remain unaffected albeit slower.[87] Many of these effects vary from person to person[91] i.e. while some individuals have high degrees of cognitive impairment with lack of sleep, in others, it has minimal effects. The exact mechanisms for the above are still unknown and the exact neural pathways and cellular mechanisms of sleep debt are still being researched.
Sleep disorders[]
- Main article: Sleep disorder
A sleep disorder, or somnipathy, is a medical disorder of the sleep patterns of a person or animal. Polysomnography is a test commonly used for diagnosing some sleep disorders. Sleep disorders are broadly classified into dyssomnias, parasomnias, and other disorders including ones caused by medical or psychological conditions and sleeping sickness. Some common sleep disorders include insomnia (chronic inability to sleep), sleep apnea (abnormally low breathing during sleep), narcolepsy (excessive sleepiness at inappropriate times), cataplexy (sudden and transient loss of muscle tone), circadian rhythm sleep disorders, and sleeping sickness (disruption of sleep cycle due to infection). Other disorders that are being studied include sleepwalking, sleep terror and bed wetting.
Studying sleep disorders is particularly useful as it gives some clues as to which parts of the brain may be involved in the modified function- this is done by comparing the imaging and histological patterns in normal and affected subjects. Treatment of sleep disorders typically involves behavioral and psychotherapeutic methods though other techniques may also be used. The choice of treatment methodology for a specific patient depends on the patient's diagnosis, medical and psychiatric history, and preferences, as well as the expertise of the treating clinician. Often, behavioral or psychotherapeutic and pharmacological approaches are compatible and can effectively be combined to maximize therapeutic benefits.
A related field is that of sleep medicine which involves the diagnosis and therapy of sleep disorders and sleep deprivation, which is a major cause of accidents. This involves a variety of diagnostic methods including polysomnography, sleep diary, multiple sleep latency test, etc. Similarly, treatment may be behavioral such as cognitive behavioral therapy or may include pharmacological medication or bright light therapy.
Dreaming[]
- Main article: Dream
{kind=link}
"The Knight's Dream", a 1655 painting by Antonio de Pereda
Dreams are successions of images, ideas, emotions, and sensations that occur involuntarily in the mind during certain stages of sleep (mainly the REM stage). The content and purpose of dreams are not yet clearly understood though various theories have been proposed. The scientific study of dreams is called oneirology.
There are many theories about the neurological basis of dreaming. This includes the activation synthesis theory- the theory that dreams result from brain stem activation during REM sleep; the continual activation theory- the theory that dreaming is a result of activation and synthesis but dreams and REM sleep are controlled by different structures in the brain; and dreams as excitations of long term memory- a theory which claims that long term memory excitations are prevalent during waking hours as well but are usually controlled and become apparent only during sleep.
There are multiple theories about dream function as well. Some studies claim that dreams strengthen semantic memories- this is based on the role of hippocampal neocortical dialog and general connections between sleep and memory. One study surmises that dreams erase junk data in the brain. Emotional adaptation and mood regulation are other proposed functions of dreaming. From an evolutionary standpoint, dreams might simulate threatening events that may be common in the animal's life and may be passed on in the form of genetic memories.[92][93] Most theories of dream function appear to be conflicting, but it is possible that many short-term dream functions could act together to achieve a bigger long-term function.[5] It may be noted that evidence for none of these theories is entirely conclusive.
The incorporation of waking memory events into dreams is another area of active research and some researchers have tried to link it to the declarative memory consolidation functions of dreaming.[94][95]
A related area of research is the neuroscience basis of nightmares. Many studies have confirmed a high prevalence of nightmares and some have correlated them with high stress levels.[96] Multiple models of nightmare production have been proposed including neo-Freudian models as well as other models such as image contextualization model, boundary thickness model, threat simulation model etc.[97] Neurotransmitter imbalance has been proposed as a cause of nightmares, as also affective network dysfunction- a model which claims that nightmare is a product of dysfunction of circuitry normally involved in dreaming.[98][99] As with dreaming, none of the models have yielded conclusive results and studies continue about these questions.
References[]
- ↑ A brief history of sleep research.
- ↑ NCBI Sleep Guide.
- ↑ Cirelli, Chiara, Shaw, Paul J; Rechtschaffen, Allan; Tononi, Giulio. {{{title}}}. Brain Research 840 (1-2): 184–193.
- ↑ Kilduff, Thomas S., Ed S. Lein, Horacio de la Iglesia, Takeshi Sakurai, Ying-hui Fu, Paul Shaw (12). New Developments in Sleep Research: Molecular Genetics, Gene Expression, and Systems Neurobiology. The Journal of Neuroscience 28 (46): 11814–11818.
- ↑ 5.0 5.1 5.2 5.3 Stickgold, Robert (2009). The Neuroscience of Sleep, 61–86, Amsterdam: Boston : Academic Press/Elsevier.
- ↑ Online Free Medical Dictionary.
- ↑ Anch, A. Michael (1988). Sleep : a scientific perspective, Englewood Cliffs, N.J.: Prentice Hall.
- ↑ Thorpy, Michael J.; Yager, Jan (2001). The encyclopedia of sleep and sleep disorders, 2nd ed., updated and rev., New York: Facts on File.
- ↑ Magnin, M., Rey, M.; Bastuji, H.; Guillemant, P.; Mauguiere, F.; Garcia-Larrea, L. (8 February 2010). Thalamic deactivation at sleep onset precedes that of the cerebral cortex in humans. Proceedings of the National Academy of Sciences 107 (8): 3829–3833.
- ↑ Jones, Edward G. (1 March 2009). Synchrony in the Interconnected Circuitry of the Thalamus and Cerebral Cortex. Annals of the New York Academy of Sciences 1157 (1): 10–23.
- ↑ Somers, VK, Dyken, ME; Mark, AL; Abboud, FM (1993-02-04). Sympathetic-nerve activity during sleep in normal subjects.. The New England Journal of Medicine 328 (5): 303–7.
- ↑ Tononi, Giulio, Cirelli, Chiara (NaN undefined NaN). Sleep function and synaptic homeostasis. Sleep Medicine Reviews 10 (1): 49–62.
- ↑ Dement, William, Kleitman, Nathaniel (1 November 1957). Cyclic variations in EEG during sleep and their relation to eye movements, body motility, and dreaming. Electroencephalography and Clinical Neurophysiology 9 (4): 673–690.
- ↑ Hughes, John R. (NaN undefined NaN). Gamma, fast, and ultrafast waves of the brain: Their relationships with epilepsy and behavior. Epilepsy & Behavior 13 (1): 25–31.
- ↑ BARKER, W, BURGWIN, S (1948 Nov-Dec). Brain wave patterns accompanying changes in sleep and wakefulness during hypnosis.. Psychosomatic Medicine 10 (6): 317–26.
- ↑ Jankel, WR, Niedermeyer, E (1985 Jan). Sleep spindles.. Journal of clinical neurophysiology : official publication of the American Electroencephalographic Society 2 (1): 1–35.
- ↑ 17.0 17.1 Hofle, N, Paus, T; Reutens, D; Fiset, P; Gotman, J; Evans, AC; Jones, BE (1997-06-15). Regional cerebral blood flow changes as a function of delta and spindle activity during slow wave sleep in humans.. The Journal of neuroscience : the official journal of the Society for Neuroscience 17 (12): 4800–8.
- ↑ OSWALD, IAN, TAYLOR, ANNE M.; TREISMAN, MICHEL (1 January 1960). DISCRIMINATIVE RESPONSES TO STIMULATION DURING HUMAN SLEEP. Brain 83 (3): 440–453.
- ↑ Loomis, A. L., Harvey, E. N.; Hobart, G. A (1938). Distribution of disturbance-patterns in the human electroencephalogram with special reference to sleep. Journal of Neurophysiology 1: 413–430.
- ↑ Dumermuth, G., Walz, W.; Scollo-Lavizzari, G.; Kleiner, B. (1 January 1972). Spectral Analysis of EEG Activity in Different Sleep Stages in Normal Adults. European Neurology 7 (5): 265–296.
- ↑ Allison, T, Van Twyver, H; Goff, WR (1972 Jul). Electrophysiological studies of the echidna, Tachyglossus aculeatus. I. Waking and sleep.. Archives italiennes de biologie 110 (2): 145–84.
- ↑ Siegel, JM, Manger, PR; Nienhuis, R; Fahringer, HM; Pettigrew, JD (1996-05-15). The echidna Tachyglossus aculeatus combines REM and non-REM aspects in a single sleep state: implications for the evolution of sleep.. The Journal of neuroscience : the official journal of the Society for Neuroscience 16 (10): 3500–6.
- ↑ Mukhametov, Lev M. (NaN undefined NaN). Unihemispheric slow-wave sleep in the Amazonian dolphin, Inia geoffrensis. Neuroscience Letters 79 (1-2): 128–132.
- ↑ Lyamin, O.I, Mukhametov, L.M; Siegel, J.M; Nazarenko, E.A; Polyakova, I.G; Shpak, O.V. Unihemispheric slow wave sleep and the state of the eyes in a white whale. Behavioural Brain Research 129 (1-2): 125–129.
- ↑ ROTH, TIMOTHY C., LESKU, JOHN A.; AMLANER, CHARLES J.; LIMA, STEVEN L. (1 December 2006). A phylogenetic analysis of the correlates of sleep in birds. Journal of Sleep Research 15 (4): 395–402.
- ↑ Mascetti, Gian Gastone, Bobbo, Daniela; Rugger, Marina; Vallortigara, Giorgio (NaN undefined NaN). Monocular sleep in male domestic chicks. Behavioural Brain Research 153 (2): 447–452.
- ↑ Rattenborg, Niels C, Lima, Steven L; Amlaner, Charles J (1 November 1999). Facultative control of avian unihemispheric sleep under the risk of predation. Behavioural Brain Research 105 (2): 163–172.
- ↑ Shaw, P. J. (NaN undefined NaN). Correlates of Sleep and Waking in Drosophila melanogaster. Science 287 (5459): 1834–1837.
- ↑ Sauer, S, Kinkelin, M; Herrmann, E; Kaiser, W (2003 Aug). The dynamics of sleep-like behaviour in honey bees.. Journal of comparative physiology. A, Neuroethology, sensory, neural, and behavioral physiology 189 (8): 599–607.
- ↑ Parmelee, Arthur H., Wenner, Waldemar H.; Schulz, Helen R. (1 October 1964). Infant sleep patterns: From birth to 16 weeks of age. The Journal of Pediatrics 65 (4): 576–582.
- ↑ 31.0 31.1 Gertner, Smadar, Greenbaum, Charles W; Sadeh, Avi; Dolfin, Zipora; Sirota, Leah; Ben-Nun, Yocheved (NaN undefined NaN). Sleep–wake patterns in preterm infants and 6 month's home environment: implications for early cognitive development. Early Human Development 68 (2): 93–102.
- ↑ Van Cauter, E. (NaN undefined NaN). Age-Related Changes in Slow Wave Sleep and REM Sleep and Relationship With Growth Hormone and Cortisol Levels in Healthy Men. JAMA: The Journal of the American Medical Association 284 (7): 861–868.
- ↑ Roffwarg, HP, Muzio, JN; Dement, WC (1966-04-29). Ontogenetic development of the human sleep-dream cycle.. Science 152 (3722): 604–19.
- ↑ Ibuka, Nobuo (NaN undefined NaN). Ontogenesis of circadian sleep-wakefulness rhythms and developmental changes of sleep in the altricial rat and in the precocial guinea pig. Behavioural Brain Research 11 (3): 185–196.
- ↑ Carskadon, MA, Wolfson, AR; Acebo, C; Tzischinsky, O; Seifer, R (1998-12-15). Adolescent sleep patterns, circadian timing, and sleepiness at a transition to early school days.. Sleep 21 (8): 871–81.
- ↑ Wolfson, Amy R., Carskadon, Mary A. (1 August 1998). Sleep Schedules and Daytime Functioning in Adolescents. Child Development 69 (4): 875–887.
- ↑ Weitzman, ED, Czeisler, CA; Coleman, RM; Spielman, AJ; Zimmerman, JC; Dement, W; Richardson, G; Pollak, CP (1981 Jul). Delayed sleep phase syndrome. A chronobiological disorder with sleep-onset insomnia.. Archives of General Psychiatry 38 (7): 737–46.
- ↑ Myers, Bryan L., Badia, Pietro (1 December 1995). Changes in circadian rhythms and sleep quality with aging: Mechanisms and interventions. Neuroscience & Biobehavioral Reviews 19 (4): 553–571.
- ↑ Borbély, Alexander A. (1 January 1998). Processes Underlying Sleep Regulation. Hormone Research 49 (3-4): 114–117.
- ↑ Mazoyer, Bernard, Houdé, Olivier; Joliot, Marc; Mellet, Emmanuel; Tzourio-Mazoyer, Nathalie (NaN undefined NaN). Regional cerebral blood flow increases during wakeful rest following cognitive training. Brain Research Bulletin 80 (3): 133–138.
- ↑ Braun, A. (NaN undefined NaN). Regional cerebral blood flow throughout the sleep-wake cycle. An H2(15)O PET study. Brain 120 (7): 1173–1197.
- ↑ McGinty, D. J., Sterman, M. B. (14 June 1968). Sleep Suppression after Basal Forebrain Lesions in the Cat. Science 160 (3833): 1253–1255.
- ↑ editor, Axel Hutt,. Sleep and anesthesia : neural correlates in theory and experiment, New York: Springer.
- ↑ Steriade, M (NaN undefined NaN). Synchronized activities of coupled oscillators in the cerebral cortex and thalamus at different levels of vigilance [published erratum appears in Cereb Cortex 1997 Dec;7(8):779]. Cerebral Cortex 7 (6): 583–604.
- ↑ Contreras, D, Destexhe, A; Sejnowski, TJ; Steriade, M (1997-02-01). Spatiotemporal patterns of spindle oscillations in cortex and thalamus.. The Journal of neuroscience : the official journal of the Society for Neuroscience 17 (3): 1179–96.
- ↑ 46.0 46.1 Revich, M., Isaacs, G.; Evarts, E.; Kety, S. (1 April 1968). THE EFFECT OF SLOW WAVE SLEEP AND REM SLEEP ON REGIONAL CEREBRAL BLOOD FLOW IN CATS. Journal of Neurochemistry 15 (4): 301–306.
- ↑ Functional neuroanatomy of human rapid eye movement sleep and dreaming.
- ↑ 48.0 48.1 Saper, Clifford B., Scammell, Thomas E.; Lu, Jun (27 October 2005). Hypothalamic regulation of sleep and circadian rhythms. Nature 437 (7063): 1257–1263.
- ↑ Siegel, Jerome M (NaN undefined NaN). The stuff dreams are made of: anatomical substrates of REM sleep. Nature Neuroscience 9 (6): 721–722.
- ↑ Nelson, JP, McCarley, RW; Hobson, JA (1983 Oct). REM sleep burst neurons, PGO waves, and eye movement information.. Journal of neurophysiology 50 (4): 784–97.
- ↑ Hobson, JA, Stickgold, R; Pace-Schott, EF (1998-02-16). The neuropsychology of REM sleep dreaming.. NeuroReport 9 (3): R1-14.
- ↑ Wilson, M., McNaughton, B. (29 July 1994). Reactivation of hippocampal ensemble memories during sleep. Science 265 (5172): 676–679.
- ↑ Stickgold, Robert, Walker, Matthew P. (NaN undefined NaN). Sleep-dependent memory consolidation and reconsolidation. Sleep Medicine 8 (4): 331–343.
- ↑ Buzsáki, G. (1 January 1996). The Hippocampo-Neocortical Dialogue. Cerebral Cortex 6 (2): 81–92.
- ↑ BuzsÁk, GyÖrgy (1 June 1998). Memory consolidation during sleep: a neurophysiological perspective. Journal of Sleep Research 7 (S1): 17–23.
- ↑ Ferrara, Michele, Moroni, Fabio; De Gennaro, Luigi; Nobili, Lino (1 January 2012). Hippocampal Sleep Features: Relations to Human Memory Function. Frontiers in Neurology 3.
- ↑ Harvard Medical School Sleep Basics.
- ↑ Siegel, Jerome H. (2002). The Neural Control of Sleep and Waking, Springer.
- ↑ 59.0 59.1 59.2 Saper, Clifford B, Chou, Thomas C; Scammell, Thomas E (1 December 2001). The sleep switch: hypothalamic control of sleep and wakefulness. Trends in Neurosciences 24 (12): 726–731.
- ↑ Lu, Jun, Sherman, David; Devor, Marshall; Saper, Clifford B. (NaN undefined NaN). A putative flip–flop switch for control of REM sleep. Nature 441 (7093): 589–594.
- ↑ Sallanon, M., Denoyer, M.; Kitahama, K.; Aubert, C.; Gay, N.; Jouvet, M. (NaN undefined NaN). Long-lasting insomnia induced by preoptic neuron lesions and its transient reversal by muscimol injection into the posterior hypothalamus in the cat. Neuroscience 32 (3): 669–683.
- ↑ Swett, CP, Hobson, JA (1968 Sep). The effects of posterior hypothalamic lesions on behavioral and electrographic manifestations of sleep and waking in cats.. Archives italiennes de biologie 106 (3): 283–93.
- ↑ Webster, Harry H., Jones, Barbara E. (NaN undefined NaN). Neurotoxic lesions of the dorsolateral pontomesencephalic tegmentum-cholinergic cell area in the cat. II. Effects upon sleep-waking states. Brain Research 458 (2): 285–302.
- ↑ Borbély, AA (1982). A two process model of sleep regulation.. Human neurobiology 1 (3): 195–204.
- ↑ Edgar, DM, Dement, WC; Fuller, CA (1993 Mar). Effect of SCN lesions on sleep in squirrel monkeys: evidence for opponent processes in sleep-wake regulation.. The Journal of neuroscience : the official journal of the Society for Neuroscience 13 (3): 1065–79.
- ↑ [edited by] Birendra N. Mallick ... [et al.]. Rapid eye movement sleep : regulation and function, Cambridge, UK: Cambridge University Press.
- ↑ McCormick, David A., Bal, Thierry (1 March 1997). SLEEP AND AROUSAL: Thalamocortical Mechanisms. Annual Review of Neuroscience 20 (1): 185–215.
- ↑ Sforza, E., Montagna, P.; Tinuper, P.; Cortelli, P.; Avoni, P.; Ferrillo, F.; Petersen, R.; Gambetti, P.; Lugaresi, E. (NaN undefined NaN). Sleep-wake cycle abnormalities in fatal familial insomnia. Evidence of the role of the thalamus in sleep regulation. Electroencephalography and Clinical Neurophysiology 94 (6): 398–405.
- ↑ Tinuper, P., Montagna, P.; Medori, R.; Cortelli, P.; Zucconi, M.; Baruzzi, A.; Lugaresi, E. (NaN undefined NaN). The thalamus participates in the regulation of the sleep-waking cycle. A clinico-pathological study in fatal familial thalamic degeneration. Electroencephalography and Clinical Neurophysiology 73 (2): 117–123.
- ↑ Coulon, P, Budde, T; Pape, HC (2012 Jan). The sleep relay--the role of the thalamus in central and decentral sleep regulation.. Pflugers Archiv : European journal of physiology 463 (1): 53–71.
- ↑ MAGOUN, HW (1952 Feb). An ascending reticular activating system in the brain stem.. A.M.A. archives of neurology and psychiatry 67 (2): 145–54; discussion 167–71.
- ↑ Mesulam, MM (1995-05-10). Cholinergic pathways and the ascending reticular activating system of the human brain.. Annals of the New York Academy of Sciences 757: 169–79.
- ↑ Foundation, editors for the Ciba; Wolstenholme, G.E.W.; O'Connor, Maeve (1961). Ciba Foundation symposium on the nature of sleep, Boston: Little, Brown.
- ↑ Krueger, James M., Obál, Ferenc; Fang, Jidong (NaN undefined NaN). Why we sleep: a theoretical view of sleep function. Sleep Medicine Reviews 3 (2): 119–129.
- ↑ KRUEGER, JAMES M., OBÄL, FERENC (1 June 1993). A neuronal group theory of sleep function. Journal of Sleep Research 2 (2): 63–69.
- ↑ Lewy, A., Wehr, T.; Goodwin, F.; Newsome, D.; Markey, S. (12 December 1980). Light suppresses melatonin secretion in humans. Science 210 (4475): 1267–1269.
- ↑ Leproult, R. (1 January 2001). Transition from Dim to Bright Light in the Morning Induces an Immediate Elevation of Cortisol Levels. Journal of Clinical Endocrinology & Metabolism 86 (1): 151–157.
- ↑ Van Cauter, E. (1 June 1992). A quantitative estimation of growth hormone secretion in normal man: reproducibility and relation to sleep and time of day. Journal of Clinical Endocrinology & Metabolism 74 (6): 1441–1450.
- ↑ Kern, W., Dodt, C.; Born, J.; Fehm, H. L. (1 January 1996). Changes in Cortisol and Growth Hormone Secretion During Nocturnal Sleep in the Course of Aging. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 51A (1): M3–M9.
- ↑ 80.0 80.1 Knutson, Kristen L., Spiegel, Karine; Penev, Plamen; Van Cauter, Eve (NaN undefined NaN). The metabolic consequences of sleep deprivation. Sleep Medicine Reviews 11 (3): 163–178.
- ↑ Spiegel, Karine, Leproult, Rachel; Van Cauter, Eve (1 October 1999). Impact of sleep debt on metabolic and endocrine function. The Lancet 354 (9188): 1435–1439.
- ↑ Cirelli, Charia, Giulio Tuononi (August 2013). Perchance to Prune. Scientific American.
- ↑ 83.0 83.1 Van Dongen, HP, Maislin, G; Mullington, JM; Dinges, DF (2003-03-15). The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation.. Sleep 26 (2): 117–26.
- ↑ Connor, Jennie Driver sleepiness and risk of serious injury to car occupants: population based case control study. British Medical Journal.
- ↑ Lim, Julian, Dinges, David F. (1 May 2008). . Annals of the New York Academy of Sciences 1129 (1): 305–322.
- ↑ WRIGHT JR., KENNETH, BADIA, PIETRO; MYERS, BRYAN; PLENZLER, STEVEN (1 March 1997). Combination of bright light and caffeine as a countermeasure for impaired alertness and performance during extended sleep deprivation. Journal of Sleep Research 6 (1): 26–35.
- ↑ 87.0 87.1 Durmer, JS, Dinges, DF (2005 Mar). Neurocognitive consequences of sleep deprivation.. Seminars in neurology 25 (1): 117–29.
- ↑ Drummond, Sean P. A., Gillin, J. Christian; Brown, Gregory G. (9 June 2001). Increased cerebral response during a divided attention task following sleep deprivation. Journal of Sleep Research 10 (2): 85–92.
- ↑ Fambrough, DM, Wolitzky, BA; Tamkun, MM; Takeyasu, K (1987 Dec). Regulation of the sodium pump in excitable cells.. Kidney international. Supplement 23 (3): S97-116.
- ↑ Tsuno, Norifumi, Besset, Alain; Ritchie, Karen (15 October 2005). Sleep and Depression. The Journal of Clinical Psychiatry 66 (10): 1254–1269.
- ↑ Chee, MW, Chuah, LY (2008 Aug). Functional neuroimaging insights into how sleep and sleep deprivation affect memory and cognition.. Current Opinion in Neurology 21 (4): 417–23.
- ↑ Revonsuo, A (2000 Dec). The reinterpretation of dreams: an evolutionary hypothesis of the function of dreaming.. The Behavioral and brain sciences 23 (6): 877–901; discussion 904–1121.
- ↑ Montangero, Jacques (2000). A more general evolutionary hypothesis about dream function. Behavioral and Brain Sciences 23 (6): 972–973.
- ↑ Stickgold, R. (NaN undefined NaN). Sleep, Learning, and Dreams: Off-line Memory Reprocessing. Science 294 (5544): 1052–1057.
- ↑ Greenberg, R, Katz, H; Schwartz, W; Pearlman, C (1992). A research-based reconsideration of the psychoanalytic theory of dreaming.. Journal of the American Psychoanalytic Association 40 (2): 531–50.
- ↑ Sadeh, Avi, Keinan, Giora; Daon, Keren (1 January 2004). Effects of Stress on Sleep: The Moderating Role of Coping Style.. Health Psychology 23 (5): 542–545.
- ↑ Nielsen, Tore, Levin, Ross (NaN undefined NaN). Nightmares: A new neurocognitive model. Sleep Medicine Reviews 11 (4): 295–310.
- ↑ Pagel, J.F. (NaN undefined NaN). Drugs, Dreams, and Nightmares. Sleep Medicine Clinics 5 (2): 277–287.
- ↑ Levin, Ross, Nielsen, Tore (1 April 2009). Nightmares, Bad Dreams, and Emotion Dysregulation: A Review and New Neurocognitive Model of Dreaming. Current Directions in Psychological Science 18 (2): 84–88.
| This page uses Creative Commons Licensed content from Wikipedia (view authors). |