Assessment |
Biopsychology |
Comparative |
Cognitive |
Developmental |
Language |
Individual differences |
Personality |
Philosophy |
Social |
Methods |
Statistics |
Clinical |
Educational |
Industrial |
Professional items |
World psychology |
Psychology: Debates · Journals · Psychologists
This article was originally an undergraduate project entitled: Recovery from Acquired Brain Injury, written by Mostly Zen (Thomas Michael) for Headway West Midlands and Newman College of Higher Education.
Introduction[]
This article was based on the report; Recovery from Acquired Brain Injury which was intended as a general guide to head injury and recovery for the non specialist (social rehabilitation workers with no formal psychology/medical training). It may also be useful to psychologists who have little training in biology. Please edit and improve this article as this is the purpose of the Psychology Wiki. However, the material reads well in the current format, so rather than move the material to separate articles or add much greater detail, it may be better to link to articles which discuss aspects of this material in more depth. Mostly Zen 20:43, 8 July 2006 (UTC)
The effect of injury on the brain is a complex subject involving a great deal of biological, cognitive and social functioning. Specialists in the rehabilitation of people with Acquired Brain Injury may not have much training or knowledge in neuron biology or brain function. Likewise, researchers in those areas may have little or no experience of working with people who are survivors of head injury. Psychologists may be very knowledgeable in the areas of cognitive functioning, but have less experience in biology or social rehabilitation. Sharing knowledge among these key areas can enhance our understanding of brain injury, and enable us to help people with brain injuries to make as full a recovery as possible, as well as to adapt and cope with those injuries which are irreparable at present.
For this reason the report was originally written, and is presented here on the Psychology Wiki for the same purposes. The cross referencing of the Psychology Wiki can help readers to understand unfamiliar terms and also allows them to explore those terms in greater depth.
Primary & Secondary Causes of Brain Injury[]
Acquired Brain Injury has a variety of causes. The most common include trauma to the head caused by traffic accidents, falls and assaults, but there are many other causes including strokes, drug overdoses and anoxia (lack of oxygen due to drowning for example).
Briefly, the brain can be damaged by any of the following:
- In trauma, the brain is violently shaken, which can cause multiple small shear type injuries across many areas of the brain, as the brain is very delicate and collides with the rough interior of the skull.
- Initial injuries can lead to swelling which causes secondary damage, as the brain encased within the skull has no room to allow for this expansion.
- Swelling can cut off the supply of oxygen to neurons (brain cells), which can then die in a matter of minutes.
- Damage to the blood vessels in the brain lining from initial trauma can also cause neuron death due to lack of oxygen.
- Blood vessels also serve as a radiator to cool the brain, overheating can cause neuron death.
- Lack of blood and oxygen trigger a chemical reaction called ischemic cascade, which is responsible for most neuron death.
- Damaged and dead neurons can release the neurotransmitters stored within their vesicles, which can over stimulate other neurons leading to further damage.
This damage to the brain, both in terms of neuron death and the severing of connections between neurons is the physiological cause of the mental impairments observed in brain injured people.
Medical advancements in preventing secondary injuries such as anoxia and ischemic cascade have lead to people surviving brain injury far more frequently than was the case in the past. This increase in frequency of survival is the reason why services such as Headway are in increasing demand. Immediate post trauma care may have become very effective in helping brain injured people to survive, but it is then necessary for the family, carers and the survivors themselves to adapt to living with the injury and attempting to recover as best as is possible – a process that will take many years or possibly the rest of their lives.
- Main article: Causes of acquired brain injury
Biological Mechanisms of Damage & Recovery[]
Damage to Neurons & Synapses[]
Neurons are the brain cells themselves, and synapses are the connections between them. Neurons send messages to each other via the synapses, and form a network of connections which allow the various areas of the brain to communicate with one another. In an uninjured brain these messages allow us to function normally, moving, talking and thinking in our everyday social lives.
By the time we are 21 we have nearly one hundred billion neurons. As we age, we lose approximately 100,000 of these a day through natural causes, leaving us with about 97% of our neurons left alive if we reached 100 years old.

Neuron image (A), diagram (B) & representation in Neural Network (C).
In the above diagram (figure i), an actual neuron is shown using a scanning electron microscope. The simplified figure shows the neuron (yellow) and the two cells in our brains which support the neuron. The Astrocyte (red) feeds the neuron oxygen and nutrients, and the Myelin cells (blue) insulate the neuron in much the same way that plastic coatings insulate electrical wires.
When a person suffers a brain injury, many neurons are destroyed and many, many more connections between the neurons are severed (because there are more connections than neurons this is always the case). This damage to the neural network is responsible for the physical, emotional, behavioural and cognitive difficulties that brain injured people suffer from.
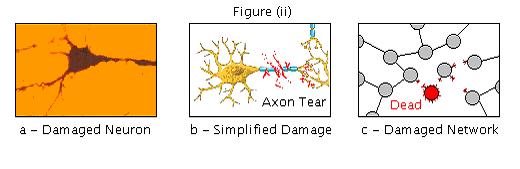
In the above diagram (figure ii), a damaged neuron is shown using an optical microscope, and damaged neurons and neural connections are shown for comparison with the healthy diagrams above.
Plasticity & Neurogenesis[]
Plasticity is the extent to which the brain can reorganise itself in terms of its neural connections (it can be reshaped, like plasticene). Synaptic plasticity is the forming of new connections both between individual neurons and between different areas of the brain. In this article, plasticity is used as an abbreviation for synaptic plasticity.
Plasticity is an on-going process that occurs in all people and can be thought of as the process which allows us to learn and grow. There are limits to plasticity however, as the brain specializes its functions into different areas, responsible for movement, vision, speech etc. If these areas are damaged, other areas can only take over their function to a limited extent.

The above new synapse is visible using green fluorescence. As new axons re-grow, they connect with the dendrites of other neurons, making new connections (blue lines). Axons re-grow at about 1mm per day until they reach about 1cm, so damage to areas greater in size than this cannot be bridged by plasticity. Also, the presence of chemicals in brain scar tissue inhibits plasticity.1&2
The other half of Plasticity is Neurogenesis. This is the recent discovery that new neurons can grow in the adult human brain.3 Although part of plasticity, it is a separate process from synaptic plasticity and so is referred to separately throughout this article.
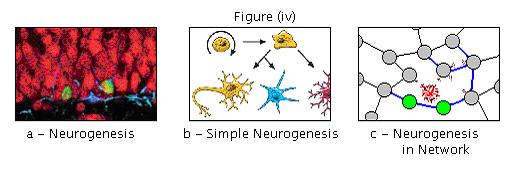
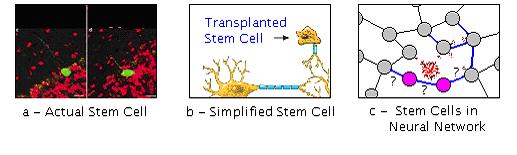
- A - Neurogenesis in the hippocampus of an adult rat (the new neurons are green).
- B - The simplified process is that stem cells produce progenitor cells, which in turn can develop into new Neurons (yellow) as well as Myelin & Astrocyte cells (blue and red respectively).
- C - In the network of neurons that makes up the brain, these new neurons may make new connections to older existing neurons (blue lines).
Although most Neurogenesis studied involves the hippocampus (a memory centre) recent research has shown Neurogenesis in the neocortex of macaque monkeys.4 The neo-cortex is responsible for higher brain function, including more human functions.
How much Recovery is Possible?[]


There are two important extremes to avoid when we are discussing brain recovery. The first is the over optimistic extreme that people with ABI can make a 100% full recovery. This kind of thinking can artificially raise people’s hopes, setting them up for future disappointment. It is also harmful in that it will prevent a brain injured person from being able to accept his or her injury and the long term effects which it will have on his or her life. It is important though to also avoid the other extreme, of pessimism.
The pessimistic view is often encountered more frequently in clients and can be a sign of accompanying psychological problems such as depression. The brain injured person may feel that he or she is ‘broken’ and beyond repair, which will be harmful to their chances of recovering some function that has been lost. Studies have shown that depression is far more common in patients with brain injury than those with other serious injuries.5 Hence depression must be dealt with, as practice and determination are necessary to regain any level of function. The two extremes are illustrated on the diagrams below, as well as the uncertain nature of recovery.


Clients displaying either of these extreme views may have trouble with insight into the nature of their injury (which may or may not be an effect of the injury itself). They may also have trouble accepting their injury even if they understand what and how the injury is and how it affects them. Either extreme is a hindrance to what recovery is possible.
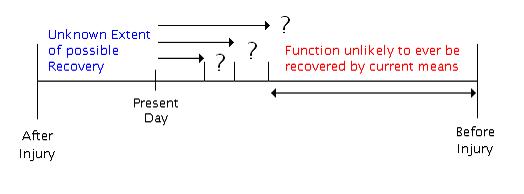
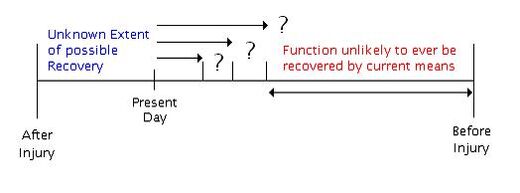
Figure (vii): The extent of recovery possible is actually unknown (although full recovery is extremely unlikely).
Different individuals recover to differing extents. This is indicated in the above figure with the question marks. Hopefully the information in this report should be helpful and enable clients to maximise any recovery that they are still able to make.
Unfortunately, the more time that has passed since the injury was inflicted, the less likely further recovery is possible. This means that most recovery will be in the initial years following the accident. The brain remains plastic throughout our lives though and so some additional recovery should remain possible. Also, as client’s age, some recovery that they may have made may be reversed due to cognitive decline in their later years, although much of this appears to be due to inactivity in terms of both exercise and mental simulation.6 However, the brain remains plastic throughout our lives (even though it is less so as we get older) and the factors which improve brain health in later sections are also invaluable in preventing cognitive decline in later life.
Theoretical Models of Recovery: Restoration & Compensation[]
These are two ways in which people can recover from brain injury. Restoration is recovery of function as it was prior to the accident, whereas Compensation is an adaptive reaction, the person changes his or her behaviour to accommodate the effects of the injury in their lives.
From a work session at Headway West Midlands, clients listed effects of ABI in seven broad categories. The table below shows how clients could potentially restore lost ability in these areas, or learn to cope with the injury if restoration is not possible.
Memory[]
Restoration Strategy
- Helping client to remember for themselves through memory games, practice mnemonics etc…
Compensation Strategy
- Keeping a diary
- Having a personal organiser/bleeper
- Keeping a daily routine
Speech[]
Restoration Strategy
- Speech therapy and every day practice.
- Recovery of Left Hemisphere (speech areas)
Compensation Strategy
- Context gesticulation and sign language.
- Learning limited speech with Right Hemisphere?
Movement[]
Restoration Strategy
- Physiotherapy, exercise
- Regaining use of right hand
Compensation Strategy
- Wheelchair, stick or frame
- Learning to use Left hand
Executive[]
Restoration Strategy
- Planning and awareness practice
Compensation Strategy
- Personal organiser or diary, keeping a routine.
Behaviour[]
Restoration Strategy
- Behaviour workshops (e.g. Anger Management)
- Considering affect on others
Compensation Strategy
- Avoiding situations in which behavioural problems normally occur. (e.g. Pub)
Emotional[]
Restoration Strategy
- Taking best action to recover in other areas will help person to feel better.
Compensation Strategy
- Learning to accept and cope with long term issues is vital to recovery
Senses[]
Restoration Strategy
- Practice use as much as possible.
- Stimulation through arts etc…
Compensation Strategy
- Sensory Aids, hearing etc
- Having a carer do cooking
- Making others aware
More recent and less severe injuries are more likely to recover via Restoration, returning to levels of cognitive ability as good or nearly as good as before. Conversely, injuries sustained a longer time ago, or those that are more severe, will be much less likely to repair fully, and so a Compensation strategy should be adopted. Although these old and/or severe injuries may not fully heal through current methods, enabling people with ABI to learn to cope practically and emotionally with their injury is a vital part of recovery.
Note that the extent of recovery discussed in the previous section may apply separately to each of the areas above. For example, full recovery emotionally and behaviourally may be possible, combined with only partial recovery of movement & speech. Also, compensation in some areas can lead to emotional restoration, i.e. as the person accepts their injuries they can be happier and live their lives less burdened.
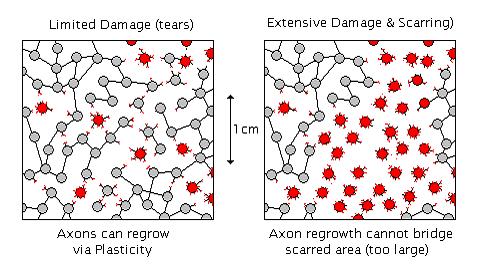
The above diagram show how limited, diffuse injury, such as axon tears from an impact type injury in which the brain is shaken, may heal more readily (through plasticity). More severe injuries from anoxia, poisoning, or open head wounds may destroy a great many neurons in a given area, which may be too large to be bridged by new axons (which grow up to 1cm on average). Understanding the extent of a brain injured persons injury is vital to understanding how much restoration of function is possible, and how much of their recovery must be due to compensation.
Practical methods to enhance recovery[]
This section will be of most practical use to Headway staff and clients. It is split into Educational, Physical and Psychological sub-sections and uses terminologies explained in the earlier sections. It is important to realise that none of these factors will help clients to regain brain function on their own. Combinations of physical (exercise, nutrition & drug use), psychological (emotional & acceptance) and educational (stimulation & social rehabilitation) will be required to make as full a recovery as possible.
Educational Factors:[]
Environmental stimulation is vital for the development of the brain in young children. There are certain critical periods during which, without environmental stimulation, children cannot ever learn speech for example. Research with animals has shown that environmental stimuli increase the rate of neurogenesis in the brain.7 & 8 Further research has shown that learning skills enhances this neurogenesis still further.9
Because brain injury itself stimulates neurogenesis and plasticity, we need to expose people with brain injury to as wide a range of environmental stimuli as possible, preferably as soon after injury as they are ready.

Art and creativity can be a great source of stimulation, especially multi sensory art-forms involving sight, hearing, touch, smell and taste. Simple activities such as pottery, painting, crafts and cookery will stimulate the mind on a variety of levels. Fig (ix): The Wholeo Dome.
There are 5 important factors10 involved in plasticity, these are:
- 1) Stimulation – Environmental & Education input is vital for new connections.
- 2) Frequency – Frequent stimulation (daily practice) is more effective.
- 3) Duration – Too short and learning is not encoded and too long causes boredom.
- 4) Intensity – Optimum arousal is the correct balance between boredom and stress.
- 5) Consistency – The same exercises or stimulation are consistently repeated.
The best time for stimulation and re-education would seem to be almost immediately post-trauma. Unfortunately this is generally not possible as the patient may be struggling to recover from physical injuries, recently come out of coma etc… However it is important to begin stimulation, practicing skills and re-education as soon as possible, so this may have implications for post traumatic care on the NHS, and also to make medical professionals, carers and clients aware of services such as Headway at an early stage.
Physical Factors:[]
Exercise[]

Exercise is good for your brain and psychological well being as well as being good for your body and general health.
Exercise has been shown to stimulate brain plasticity in mammals.12 It has also been shown to increase information processing ability in the brain, and to be a protective factor in reducing cognitive decline in old age.13
Exercise naturally releases endorphins (our bodies natural painkillers). Endorphins are mimicked by Opiate type drugs, which have also been shown to stimulate neurogenesis in rats.14 This suggests that the endorphins released during exercise may in fact stimulate neurogenesis in our brains, as the endorphins have similar biological function as the opiates. Endorphins are better for us in fact, because opiates (e.g. heroin) are dangerously addictive. Some people even claim to be addicted to the natural endorphin high that exercise can give.
Apart from this, exercise is good for our general health by being stress relieving and good for our heart and circulation. Improved circulation is indirectly beneficial to the brain by ensuring adequate flow of nutrients and oxygen.
Physiotherapy[]
This will differ from conventional physiotherapy following a physical injury to the body. In this case, it is the stimulation to the injured areas of the brain (and connected areas), rather than the limb itself which is important in recovery. The way in which the physiotherapy is carried out however, may be indistinguishable from normal physiotherapy.
Research has been carried out with Squirrel Monkeys11 in which the part of their brain which controls their right hand was deliberately damaged (similar to stroke injury). As expected, the monkey’s control of that hand was severely impaired. The researchers then split the monkeys into two groups. One group was allowed to use either hand, and tended to use their unimpaired hand (compensation) showing little recovery of their weaker hand when forced to use it. The other group were forced to use their weaker hand, and seemed to show quite good recovery of function over 12 weeks (restoration). When the parts of their brain were scanned afterwards, the part of the brain responsible for controlling the arm and elbow seemed to have taken over some of the hand control in the improved monkeys.
This means that although people with ABI might not want to use weaker limbs or practice skills that they find difficult, that restoration of function may only be possible through practice.
Movement Problems[]
Many clients may have problems with movement which make vigorous exercise difficult if not impossible. Alternative forms of exercise such as swimming, gardening or even walking briskly for as little as 30 minutes a day can still be very beneficial however. Clients should be encouraged to exercise whenever possible.
Nutrition[]
This section is covered in far greater detail in Appendix 2.
CARBOHYDRATES: Responsible for our energy levels throughout the day, the best carbohydrates to eat are those with a low or moderate glycaemic index, such as fruits, whole grains, and sweet potatoes. These give our body and brain a slow trickle of energy throughout the day which should aid concentration.
PROTEINS: Proteins build our bodies but also make the neurotransmitters that send messages between our neurons. There are more neurotransmitters than can be discussed in detail here but two important ones are Serotonin (5HT) and Dopamine (DA).
Foods which provide building blocks for these neurotransmitters are discussed in the appendix.
FATS: Saturated fats and artificial hydrogenated oils have been shown to be harmful to the plasticity of the brain15 which will impede brain repair following ABI. This means it is especially important that people with ABI reduce these fats from their diet, apart from the fact that these fats lead to furring of the arteries in all people, which increases risk of stroke.
VITAMINS & MINERALS: Vitamin C is especially important in the brain, where it is present ten times more concentrated than the rest of the body. Vitamin C is a powerful anti oxidant, which helps to reduce damage to neurons from free radicals, and may even have a role in protecting the brain from trauma damage.16
Drugs & Alcohol[]
It is beyond the scope of this report to examine the effects of drugs and alcohol in much detail, however the appendices contain a client work session plan on the three most commonly used recreational drugs. Clients and carers should be made aware that substances that are detrimental to physical health are also detrimental to the health of our brains.
Psychological Factors:[]
Psychological factors can inhibit recovery of brain function, and in many cases psychological factors may be the most difficult aspect of the injury for the affected person to deal with. Long term studies (over 50 years) with brain injured veterans from World War II have shown that people with ABI are more than 50% more likely to suffer from depression than veterans with other injuries (who also suffer depression more frequently than the rest of the population).17 In addition, people with ABI suffer from sleep disturbances far more frequently than the rest of the population18, due to disturbed chemical processes which naturally occur during sleep. Disturbed sleep is also a major cause of depression.
Both depression and poor sleep cause people trouble in concentration, memory and moods. Some of the cognitive affects attributed to head injury may in fact be due to accompanying psychological causes, even if the cause of these problems was the initial physical injury.
Depression causes people to have a negative outlook on life, and may cause depressed people with ABI to adopt the negative extreme of feeling ‘broken’ and to feel that any recovery is impossible. One does encounter this with Headway clients, some of whom even go so far as to say they wish they had died in their accident. These clients need help to accept the injury in their lives. On the positive side, some clients report that they feel they are a changed or better person since their accident, as they no longer engage in negative or harmful behaviours which they used to prior to injury.
Treatment for depression is somewhat outside the scope of this report, but counselling for the client, enabling them to accept the affects of their injury and gain insight into how they can cope with the injury and get on with their lives. Counselling may also be needed due to personality changes following the injury, as well as social and relationship difficulties which may be faced trying to cope with the change.
Medication may also be useful as current theories suggest that depression is either due to, or a cause of diminished plasticity in the brain19 especially the hippocampus which is associated with memory function.
Possible Future therapeutic & medical intervention[]
This section will not yet be of practical use, as the therapies described are still being researched and developed. Whilst most testing at this stage is being conducted on animals, at some point human volunteers will be needed to test these therapies. It is likely in the next 10-20 years or so, that clients with ABI will be approached to undergo these new techniques that are being pioneered, which is why this section has been included. Future forms of medical intervention will likely focus on increasing Neurogenesis in the brain. This will take one of the following forms:
- 1) Transplanting neurons or stem cells (using therapeutic cloning or otherwise).
- 2) Increasing the rate of neurogenesis (or preventing its inhibition) through medical drugs.
Transplantation[]
In transplantation there are two possibilities. The first is transplanting an adult neuron from a donor. Researchers have managed to transplant neurons from one animal’s brain into another, and have also observed the growth of new axons to form synapses between transplanted neurons and original ones. For example, pig neurons have been successfully transplanted into a rat brain.20 In theory the same process should be possible transplanting neurons from a human donor brain into an injured brain. However the idea of having someone else’s brain cells in your head may be more unsettling than the idea of having a donor’s kidney for example.
The second possibility of transplantation is that of transplanting stem cells. Stem cells are undifferentiated cells, which we all have in our bodies. They can become any type of cell in the body, and become the correct type of cell by the presence of nearby mature cells signalling what type of cell is required. Neural stem cells are what cause natural neurogenesis, the type stimulated by exercise and mental stimulation. Transplantation of these naturally occurring cells to the damaged areas in the brain could greatly speed recovery.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Stem cells also occur in different parts of our bodies, such as in our bone marrow. In the above diagram, transplanted stem cells taken from bone marrow are observed to differentiate into different types of brain cell and fuse with existing cells.21
Much controversy surrounds stem cells because of one method of producing them known as therapeutic cloning. This involves making a clone embryo using the patients DNA. Recently a scientist called Hwang Woo-suk was found to have fraudulently claimed to have created stem cells from cloned embryos.22 Had this been true it would have been very important for treatment of patients with paralysis and brain injury. Apart from fraudulent claims, many people are opposed to therapeutic cloning on the basis that they consider the embryos to be human beings and see using them to harvest stem cells as killing. Whether future stem cell therapies use cloned stem cells or stem cells from bone marrow remains to be seen.
Drug Intervention[]
Hamsters see again (23)
Cannabis[]
As cannabis is a commonly used drug in our society, it is hardly surprising that some people with ABI use the drug. The author was asked to research the effects of the drug because certain clients at Headway West Midlands are known to use it. Research in the area has found several different results. A study in 2005 has shown that Cannabinoids (cannabis like drugs) actually promote neurogenesis in the adult hippocampus (a memory area), and that anti anxiety and anti-depressant effects may be due to this neurogenesis.24 However, another study in 2001 showed that cannabinoids inhibit the growth of new synapses (plasticity) in the hippocampus.25 What overall effect these two conflicting effects cause is unknown, but it is widely known that cannabis inhibits memory formation. Future medicines derived from the drug may be beneficial in short term doses (due to the increased neurogenesis) but counterproductive if taken for long periods (due to inhibiting plasticity and memory).
Other affects of cannabinoids are that they are potent anti oxidants (like Vitamin C) except easily able to cross the blood brain barrier. However, since cannabis is normally smoked, the harmful affects of smoking will likely overwhelm and positive affect. Again the possibility of future medicines is here.
Unwanted Side Effects[]
Artificially increasing plasticity, both synaptic plasticity and neurogenesis could have undesirable side effects, as could implantation of neurons or stem cells. The new cells and the connections between them are not certain to form connections as desired to restore lost function, although in combination with stimulation and re-education therapies this seems more likely. Unintended changes in plasticity may be a cause of conditions such as schizophrenia, according to recent theories of the illness.
Many new connections may be formed that were not intended, which may cause changes in that persons personality, an effect which is also caused by head injury, and one which carers find very difficult to deal with emotionally. Clearly the risks must be balanced with the benefits.
See Also[]
External Links[]
Primary & Secondary causes of Brain Injury[]
http://en.wikipedia.org/wiki/NINDS_brain_trauma_research
Biological Mechanisms of Damage & Recovery[]
- Life & Death of a Neuron: http://helpforheadaches.com/articles/nihsheets/life-neuron.htm
- Plasticity: http://en.wikipedia.org/wiki/Plasticity_(brain)
- 2011 Paper from Brain Journal on Plasticity: http://brain.oxfordjournals.org/content/134/6/1591.full
Neurogenesis: http://en.wikipedia.org/wiki/Neurogenesis
How much recovery is possible?[]
Factors known to influence recovery in clear layman language:
http://www.how-psychology-tests-brain-injury.com/brain-injury-recovery.html
Depression as extreme view: http://www.adap.net/tbi/depression.pdf
Theoretical Models of Recovery: Restoration & Compensation[]
- Restoration vs. Compensation Note that the term Restoration is sometimes referred to as Restitution elsewhere.
Practical methods to enhance Recovery[]
- Educational – Stimulation
- Physical – Exercise (Neurogenesis) http://www.fi.edu/brain/exercise.htm
- Nutrition – Brain Health: http://sln.fi.edu/brain/pyramid.htm
http://sln.fi.edu/brain/fats.htm
- Mental health link to Diet Change http://news.bbc.co.uk/1/hi/health/4610070.stm
- Psychological – Depression http://news.bbc.co.uk/1/hi/health/3370411.stm
Possible Future therapeutic / medical intervention[]
- Nanotech helps blind hamsters see: http://news.bbc.co.uk/1/hi/sci/tech/4801728.stm
- Cambridge Centre for Brain Repair: http://www.brc.cam.ac.uk/
- Foetal stem cells: http://www.npr.org/templates/story/story.php?storyId=5195551
References[]
These references are all cited in the main article.
- [1] Tan, Andrew M.; Zhang, Weibing; Levine, Joel M. (2005) NG2: a component of the glial scar that inhibits axon growth. Journal of Anatomy. 207(6):717-725, December 2005
- [2] Fawcett, James. W & Asher, Richard. A. (1999) The Glial Scar and Central Nervous System Repair. Brain Research Bulletin Vol 49 No 6. pp 377-391. Elsevier Science Inc.
- [3] Eriksson, P. S., E. Perfilieva, T. Bjork-Eriksson, A. M. Alborn, C. Nordberg, D. A. Peterson and F. H. Gage. 1998. Neurogenesis in the adult human hippocampus. Nature Medicine 4:1313-1317.
- [4] Gould, Elizabeth *; Reeves, Alison J.; Graziano, Michael S. A.; Gross, Charles G. (1999) Neurogenesis in the Neocortex of Adult Primates. Science. 286(5439):548-552, October 15, 1999.
- [5] Ricardo E. Jorge, MD; Robert G. Robinson, MD; David Moser, PhD; Amane Tateno, MD; Benedicto Crespo-Facorro, MD; Stephan Arndt, PhD. (2004) Major Depression Following Traumatic Brain Injury. Arch Gen Psychiatry. 2004;61:42-50.
- [6] Sitskoorn, Margriet M. (2005). The plasticity of the brain: The effect of behaviour. Psycholoog. Vol 40(5) May 2005, 262-267.
- [7] Kempermann G, Kuhn HG, Gage FH. 1997. More hippocampal neurons in adult mice living in an enriched environment. Nature 386: 493-495.
- [8] Kempermann G, Brandon EP, Gage FH. (1998) Environmental stimulation of 129/SvJ mice causes increased cell proliferation and neurogenesis in the adult dentate gyrus. Curr Biol. 1998 Jul 30-Aug 13;8(16):939-42.
- [9] Gould, Elizabeth; Beylin, Anna; Tanapat, Patima; Reeves, Alison; Shors, Tracey J. (1999) Learning enhances adult neurogenesis in the hippocampal formation. Nature Neuroscience. Vol 2(3) Mar 1999, 260-265.
- [10] EDUCATION Continuous stimulation is better than hard core 4 hours a week
- [11] Frost, S. B; Barbay, S; Friel, K. M; Plautz, E. J; Nudo, R. J. (2003). Reorganization of Remote Cortical Regions After Ischemic Brain Injury: A Potential Substrate for Stroke Recovery. Journal of Neurophysiology. Vol 89(6) Jun 2003, 3205-3214.
- [12] Kleim J.A, Jones T. A & Schallert T (2003) Motor Enrichment and the Induction of Plasticity before or after Brain Injury. Neurochemical Research. 28(11):1757-1769, Kluwer Academic Publishers.
- [13] Cotman, C. W & Engesser-Cesar, C. (2002) Exercise Enhances and Protects Brain Function. Exercise & Sport Sciences Reviews. 30(2):75-79, April 2002. 2002 The American College of Sports Medicine
- [14] Persson AI, Harlan T, Bull C, Zarnegar P, Ekman R, Terenius L, Eriksson PS. (2003) Mu- and delta-opioid receptor antagonists decrease proliferation and increase neurogenesis in cultures of rat adult hippocampal progenitors. European Journal of Neuroscience, 2003 Mar;17(6):1159-72
- [15] Wu A, Molteni R, Ying Z, Gomez-Pinilla F. (2003) A saturated-fat diet aggravates the outcome of traumatic brain injury on hippocampal plasticity and cognitive function by reducing brain-derived neurotrophic factor. Neuroscience. 2003;119(2):365-75. Medline
- [16] Rice, Margaret E. (2000). Ascorbate regulation and its neuroprotective role in the brain. Trends Neurosci. (2000) 23, 209–216
- [17] Holsinger, Tracey MD; Steffens, David C. MD; Phillips, Caroline MS; Helms, Michael J. MS; Havlik, Richard J. MD, MPH; Breitner, John C. S. MD, MPH; Guralnik, Jack M. MD, PhD; Plassman, Brenda L. PhD (2002) Head Injury in Early Adulthood and the Lifetime Risk of Depression. Archives of General Psychiatry. 59(1):17-22, January 2002.
- [18] Clinchot, Daniel M; Bogner, Jennifer; Mysiw, W. Jerry; Fugate, Lisa; Corrigan, John. (1998). Defining Sleep Disturbance after Brain Injury. Journal of Physical Medicine & Rehabilitation. 77(4):291-295, July/August 1998.
- [19] Kempermann, Gerd; Kronenberg, Golo. (2003) Depressed new neurons--adult hippocampal neurogenesis and a cellular plasticity hypothesis of major depression. Biological Psychiatry. Vol 54(5) Sep 2003, 499-503.
- [20] Deacon T, Whatley B, LeBlanc C, Lin L, Isacson O. (1999) Pig fetal septal neurons implanted into the hippocampus of aged or cholinergic deafferented rats grow axons and form cross-species synapses in appropriate target regions. Cell Transplant. 1999 Jan-Feb;8(1):111-29. Medline
- [21] James M. W, Clas B. J, Angelica T & Helen M. B. (2003) Stable reprogrammed heterokaryons form spontaneously in Purkinje neurons after bone marrow transplant. Nature Cell Biology 5, 959 - 966 (2003). Published online. Web page accessed 28/02/06
- [22] Journal Retracts Hwan Woo-Suk Research Papers. Web page accessed 15/03/06
- [23] Hamsters See again! - Need BBC article link
- [24] Wen Jiang, Yun Zhang, Lan Xiao, Jamie Van Cleemput, Shao-Ping Ji, Guang Bai and Xia Zhang. (2005). Cannabinoids promote embryonic and adult hippocampus neurogenesis and produce anxiolytic- and antidepressant-like effects. J. Clin. Invest. 115:3104-3116 (2005).
- [25] Kim, Daniel & Thayer, Stanley A. (2001) Cannabinoids Inhibit the Formation of New Synapses between Hippocampal Neurons in Culture. The Journal of Neuroscience, 2001, 21:RC146:1-5
- Medley,A. & Worthington, A. (2007) Keeping up with our clients:Self-regulation in brain injury. Clinical Psychology Forum, 175, 37-40
Picture References[]
(Unless otherwise noted, all diagrams were illustrated by the author)
Photographs of staff and clients taken from Headway West Midlands website: http://www.headway-wm.org.uk/ Web page accessed 16/03/06
- Figure (i): a – Actual Neuron (scanning electron microscope image)
Professor Willman’s personal pages at Viterbo University website http://www.viterbo.edu/personalpages/faculty/DWillman/p431_neural.htm Web page accessed 23/02/06
- Figure (ii): a – Damaged Neuron
Neurostructural Research Laboratories http://www.neurostructural.org/applications.htm Web page accessed 25/02/06
- Figure (iii): a – Actual New Synapse
MIT Open-courseware: Department of Brain & Cognitive Sciences http://ocw.mit.edu/OcwWeb/Brain-and-Cognitive-Sciences/9-301JNeural-Plasticity-in-Learning-and-DevelopmentSpring2002/CourseHome/ Web page accessed 23/02/06
- Figure (iv): a – Actual Neurogenesis
Scandinavian Life Science Journal: Neurogenesis in rat hippocampus. http://www.life-science.se/2005_1_6.htm Web page accessed 20/02/06
- ‘Simplified’ parts of above 4 diagrams adapted from pictures from:
NIH Publication No.02-3440d National Institute of Neurological Disorders & Stroke http://helpforheadaches.com/articles/nihsheets/life-neuron.htm Web page accessed 18/02/06
- Figure (ix) The Wholeo Dome
From Wholeo Online by Caroling www.wholeo.net Web page accessed 22/02/06
- Figure (x)
Transplanted cells fuse with existing neurons Nature Journal Online http://www.nature.com/ncb/journal/v5/n11/thumbs/ncb1053-f7.jpg Web page accessed 28/02/06