| ||||||||||||||||
Autism is classified as a complex neurodevelopmental condition that includes marked peculiarities or impairments with social interaction and communication skills, combined with rigid, repetitive behaviors and sensory processing difficulties. It is mostly considered a spectrum condition, due to its widely variable range of symptoms and severity, hence its official name autism spectrum disorder. The condition also can cause significant challenges with learning, reasoning, motor skills, behavior, interpersonal and executive functioning, emotional development, interpretation and sensory regulation.
Although the specific etiology of autism is unknown, many researchers suspect that autism results from genetically mediated vulnerabilities to environmental triggers. Furthermore, while there is disagreement about the magnitude, nature, and mechanisms for such environmental factors, researchers have found at least seven major genes prevalent among individuals diagnosed as autistic. The CDC estimates that autism occurs in as many as one United States child in 68. For families that already have one autistic child, the odds of a second autistic child may be as high as one in twenty. Diagnosis is based on a list of psychiatric criteria, and a series of standardized clinical tests may also be used.

{kind=link}
Autistic art depicting a young woman spinning in a dress
Autism may not be physiologically obvious. A complete physical and neurological evaluation will typically be part of diagnosing autism. Autism is now generally considered a spectrum condition.
By definition, autism must manifest delays in "social interaction, language as used in social communication, or symbolic or imaginative play," with "onset prior to age 3 years", according to the Diagnostic and Statistical Manual of Mental Disorders. The ICD-10 also says that symptoms must "manifest before the age of three years." There have been large increases in the reported incidence of autism, for reasons that are heavily debated by researchers in psychology and related fields within the scientific community.
Some children with autism have improved their social and other skills to the point, where they can fully participate in mainstream education and social events, but there are lingering concerns that an absolute cure from autism is impossible with current technology. However, many autistic children and adults who are able to communicate (at least in writing) are opposed to attempts to cure their conditions, and see such conditions as part of who they are.
History[]

Dr. Hans Asperger described a form of autism in the 1940s that later became known as Asperger's syndrome.
The word autism was first used in the English language by Swiss psychiatrist Eugene Bleuler in a 1912 number of the American Journal of Insanity. It comes from the Greek word for "self".
However, the classification of autism did not occur until the middle of the twentieth century, when in 1943 psychiatrist Dr. Leo Kanner of the Johns Hopkins Hospital in Baltimore reported on 11 child patients with striking behavioral similarities, and introduced the label early infantile autism. He suggested "autism" from the Greek αυτος (autos), meaning "self", to describe the fact that the children seemed to lack interest in other people. Although Kanner's first paper on the subject was published in a (now defunct) journal, The Nervous Child, almost every characteristic he originally described is still regarded as typical of the autistic spectrum of disorders.
At the same time an Austrian scientist, Dr. Hans Asperger, described a different form of autism that became known as Asperger's syndrome—but the widespread recognition of Asperger's work was delayed by World War II in Germany, and by the fact that his seminal paper wasn't translated into English for almost 50 years. The majority of his work wasn't widely read until 1997.
Thus these two conditions were described and are today listed in the Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR (fourth edition, text revision 1) as two of the five pervasive developmental disorders (PDD), more often referred to today as autism spectrum disorders (ASD). All of these conditions are characterized by varying degrees of difference in communication skills, social interactions, and restricted, repetitive and stereotyped patterns of behavior.
Few clinicians today solely use the DSM-IV criteria for determining a diagnosis of autism, which are based on the absence or delay of certain developmental milestones. Many clinicians instead use an alternate means (or a combination thereof) to more accurately determine a diagnosis.
Terminology[]
Over 80% of autistic adults prefer to be called "autistic people" instead of "people with autism" (person-first terminology).[1] The autistic community generally prefers the term autistic. They argue that autism is not a tragedy or a thing that can be separated from an individual.[2] This article uses the term autistic (see talk page).
The intense interests of autistic people are sometimes called "special interests."
"Stimming" is a shortened term to describe self-stimulatory behavior.
Characteristics[]

Dr. Leo Kanner introduced the label early infantile autism in 1943.
There is a great diversity in the skills and behaviors of autistic people, and physicians will often arrive at different conclusions about the appropriate diagnosis. Much of this is due to the sensory system of an autistic which is quite different from the sensory system of other people, since certain stimulations can affect an autistic differently than a non-autistic, and the degree to which the sensory system is affected varies wildly from one autistic person to another.
Nevertheless, professionals within pediatric care and development often look for early indicators of autism in order to initiate treatment as early as possible. Treatment for autism can be controversial. Some people do not believe autism itself is a disorder, and some raise concerns over certain treatments doing more harm than good.
Social development[]
The social development of autistic people greatly varies. Some have severe difficulties while others have subtler ones.
Typically developing infants are social beings—early in life they do such things as gaze at people, turn toward voices, grasp a finger, and even smile. In contrast, many autistic children prefer objects to faces and may have mild to severe difficulties learning to engage in the give-and-take of everyday human interaction. Some children appear indifferent from an early age because they avoid eye contact and are less interactive than typically-developing children.
Some autistic children find affection overwhelming. They may passively accept it or resist it. They may not seek comfort from others and may not respond to their parents' moods in typical ways. Parents who looked forward to the joys of cuddling, teaching, and playing with their child may feel crushed by this lack of expected attachment behavior. Research has suggested that although autistic children are attached to their parents, their expression of this attachment is unusual and difficult for non-autistic people to interpret.
Some autistic children have delayed development of "theory of mind", the ability to see things from another person's perspective. This ability typically shows up in humans above the age of five. Autistic people find it harder to understand people's different knowledge, feelings, and intentions. Reading social cues like gestures and facial expressions is more difficult. This can lead to intense social alienation, and many autistic children may create imaginary friends as companionship. However, having an imaginary friend is not necessarily a sign of autism and also occurs in non-autistic children.
Some autistic people learn to mask their autism. This includes behavior like suppressing the need to stim, pretending to be happy when they feel uncomfortable, and memorizing how to respond in social situations. However, fitting in comes with a profound cost. Masking is associated with anxiety, depression, suicidality, and other issues.[3][4][5] Experiencing autism acceptance can improve mental health.[6][7] A supportive environment may help autistic people feel more comfortable being themselves.[8]
Communication differences and difficulties[]
Degree of communication difficulties varies greatly among autistic people.
Some autistic children show communication difficulties in early childhood. Others develop typically at first, then stop or regress. Some children may exhibit only slight delays in language, or even seem to have precocious language and unusually large vocabularies, but have great difficulty in sustaining typical conversations.
Unmet communication needs can cause frustration, stress, and reduced quality of life. If an autistic person can't express their needs in a way others understand, it can lead to outbursts and desperate attempts to communicate. Adequate support for communication skills (whether speech or an alternative option like sign language) is crucial for wellbeing.
Speaking skills[]
Some autistic people are nonspeaking or have a limited ability to speak. Many of these people are fully literate and may gain speech skills as late as the teenage years. Forms of augmentative and alternative communication like tablet apps, sign language, and typing can help them express their thoughts and feelings. Many nonspeaking people are intelligent and aware. They may frequent online discussion boards and seek out other autistic people online.
Autistic speakers may use language in idiosyncratic ways and have delayed language use. Some have speech disorders such as stuttering. Their tone of voice may be high-pitched, sing-song, or flat, robot-like voice is common in autistic children. Some autistic children speak like "little professors" with a factual tone.
Some autistic people repeat words or phrases, a condition called echolalia. Echolalia can be used for enjoyment, to enhance focus, for self-soothing, or for communication.
It is important to note that autistic people with limited or no speech abilities can usually understand what is being said around them.
Conversation skills[]
Handling the "give and take" of typical conversations can be difficult for autistic people. Autistic people may enjoy monologuing about their favorite subjects. When speaking with each other, autistic people may engage in "parallel monologue"—taking turns expressing views and information.
Autistic people may struggle to understand the meaning of voice inflections, subtext, facial expressions, and body language.
Double empathy problem[]
The "double empathy problem" describes how it is harder for non-autistic and autistic people to relate to each other.[9][10][11][12] Non-autistic people tend to judge autistic people more harshly than they judge non-autistic people.[13][14] However, they are less judgmental when they know the person is autistic and when they understand autism better,[15] suggesting that improving understanding of autism could help.
Autistic people tend to speak literally and say what they mean. Non-autistic people rely more on subtext and hidden meanings. These differences mean that autistic people may not pick up on subtext from non-autistics, while non-autistics make false assumptions about subtext when the autistic person did not intend any.
Repetitive behaviors[]


{kind=link}
Stim toys owned by an autistic woman
Repetitive motions, known as self-stimulation or "stimming," are common in autistic people. They may be subtle, like tapping a pencil or shaking a leg, or noticeable, like hand-flapping and rocking. Autistic people report that these behaviors help with self-regulation.[16] Some researchers and autistic advocates have argued that preventing people from stimming is harmful and that non-injurious stimming should be accepted.[17][18]
Some autistic people enjoy punding (lining up objects). Autistic adults have described it as relaxing.[19] Interfering with their arrangements can upset them.
Many autistic people need routine to feel secure. Changes to daily routine can feel distressing and disorienting. Coping with unpredictability can be extremely difficult for some autistic people.
Many autistic people experience deep, narrow interests. Examples include vacuum cleaners, infrastructure, Chinese history, and writing poetry. Engaging with these interests can be a source of joy, relaxation, and skill development.
Sensory system[]


{kind=link}
Auditory sensitivity depicted by autistic artist Luna Rose
Sensory integration dysfunction is common in autistic people. This can manifest in different ways. These include oversensitivity or underreactivity to touch, movement, sights, or sounds; physical clumsiness or carelessness; poor body awareness; a tendency to be easily distracted; impulsive physical or verbal behavior; an activity level that is unusually high or low; not unwinding or calming oneself; difficulty learning new movements; difficulty in making transitions from one situation to another; social and/or emotional problems; delays in speech, language or motor skills; specific learning difficulties/delays in academic achievement.
Sensitive hearing is a common struggle. Autistic people may struggle to filter out background noises, such as in a large crowd of people (see cocktail party effect). Loud sounds, such as noises from blenders or motorcycles, may be distracting or painful.
Sensory difficulties were not part of the DSM-IV diagnostic criteria. They have been added in the DSM-5.
Other traits[]
Autistic people may struggle with sensory and emotional regulation. They may lead to crying and outbursts under stress. Loss of predictability is a common trigger. Excessive stress can cause intense self-stimulatory behavior, self-injury, aggression, or withdrawal.
Educational support needs[]
Autistic students can face challenges in classroom settings. Background noise, social nuances, and stigma may be difficult to navigate. They may not know how to understand or befriend their peers.
Some autistic students benefit from special education, while others may attend mainstream classes with support.
Ways to support autistic students include:[20]
- Visual schedules to help them anticipate the day's activities and make transitions easier
- Social stories to prepare them for new or challenging situations
- A quiet place to take breaks
- Fidget tools for stimming
- Sensory-blocking options like headphones or study carrels
- A peer mentor or "buddy"
- Taking tests in a separate, quiet room
- Integrating special interests into lessons
- Teacher's aides for additional support
Some autistic children may find working in pairs helpful so they can make friends. Others find paired work more stressful than working solo.
Reducing stress at school is important for success.
Teaching social and emotional concepts using systematic teaching approaches such as The Incredible 5-Point Scale or other Cognitive Behavioral strategies can help.
DSM definition[]
DSM-V[]
Autism is defined in section 299.00 of the DSM-V as:
A. Persistent deficits in social communication and social interaction across multiple contexts, as manifested by the following, currently or by history.
1. Deficits in social-emotional reciprocity, ranging, for example, from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
2. Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures; to a total lack of facial expressions and nonverbal communication.
3. Deficits in developing, maintaining, and understanding relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
Specify current severity:
Severity is based on social communication impairments and restricted repetitive patterns of behavior.
B. Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following, currently or by history (examples are illustrative, not exhaustive; see text):
1. Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypies, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns or verbal nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat food every day).
3. Highly restricted, fixated interests that are abnormal in intensity or focus (e.g, strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interest).
4. Hyper- or hyporeactivity to sensory input or unusual interests in sensory aspects of the environment (e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
Specify current severity:
Severity is based on social communication impairments and restricted, repetitive patterns of behavior.
C. Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).
D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.
Note: Individuals with a well-established DSM-IV diagnosis of autistic disorder, Asperger’s disorder, or pervasive developmental disorder not otherwise specified should be given the diagnosis of autism spectrum disorder. Individuals who have marked deficits in social communication, but whose symptoms do not otherwise meet criteria for autism spectrum disorder, should be evaluated for social (pragmatic) communication disorder.
Specify if: With or without accompanying intellectual impairment With or without accompanying language impairment Associated with a known medical or genetic condition or environmental factor (Coding note: Use additional code to identify the associated medical or genetic condition.) Associated with another neurodevelopmental, mental, or behavioral disorder (Coding note: Use additional code[s] to identify the associated neurodevelopmental, mental, or behavioral disorder[s].) With catatonia (refer to the criteria for catatonia associated with another mental disorder, pp. 119-120, for definition) (Coding note: Use additional code 293.89 [F06.1] catatonia associated with autism spectrum disorder to indicate the presence of the comorbid catatonia.)
The DSM-5 offers 3 severity levels. A person's levels may change over time.
| Severity level | Social communication | Restricted, repetitive behaviors |
| Level 3
"Requiring very substantial support” |
Severe deficits in verbal and nonverbal social communication skills cause severe impairments in functioning, very limited initiation of social interactions, and minimal response to social overtures from others. For example, a person with few words of intelligible speech who rarely initiates interaction and, when he or she does, makes unusual approaches to meet needs only and responds to only very direct social approaches | Inflexibility of behavior, extreme difficulty coping with change, or other restricted/repetitive behaviors markedly interfere with functioning in all spheres. Great distress/difficulty changing focus or action. |
| Level 2
"Requiring substantial support” |
Marked deficits in verbal and nonverbal social communication skills; social impairments apparent even with supports in place; limited initiation of social interactions; and reduced or abnormal responses to social overtures from others. For example, a person who speaks simple sentences, whose interaction is limited to narrow special interests, and how has markedly odd nonverbal communication. | Inflexibility of behavior, difficulty coping with change, or other restricted/repetitive behaviors appear frequently enough to be obvious to the casual observer and interfere with functioning in a variety of contexts. Distress and/or difficulty changing focus or action. |
| Level 1
"Requiring support” |
Without supports in place, deficits in social communication cause noticeable impairments. Difficulty initiating social interactions, and clear examples of atypical or unsuccessful response to social overtures of others. May appear to have decreased interest in social interactions. For example, a person who is able to speak in full sentences and engages in communication but whose to- and-fro conversation with others fails, and whose attempts to make friends are odd and typically unsuccessful. | Inflexibility of behavior causes significant interference with functioning in one or more contexts. Difficulty switching between activities. Problems of organization and planning hamper independence. |
DSM-IV[]
Autism is defined in section 299.00 of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) as:
- A total of six (or more) items from (1), (2) and (3), with at least two from (1), and one each from (2) and (3):
- qualitative impairment in social interaction, as manifested by at least two of the following:
- marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction
- failure to develop peer relationships appropriate to developmental level
- a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g., by a lack of showing, bringing, or pointing out objects of interest)
- lack of social or emotional reciprocity
- qualitative impairments in communication as manifested by at least one of the following:
- delay in, or total lack of, the development of spoken language (not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime)
- in individuals with adequate speech, marked impairment in the ability to initiate or sustain a conversation with others
- stereotyped and repetitive use of language or idiosyncratic language
- lack of varied, spontaneous make-believe play or social imitative play appropriate to developmental level
- restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following:
- encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus
- apparently inflexible adherence to specific, nonfunctional routines or rituals
- stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements)
- persistent preoccupation with parts of objects
- qualitative impairment in social interaction, as manifested by at least two of the following:
- Delays or abnormal functioning in at least one of the following areas, with onset prior to age 3 years: (1) social interaction, (2) language as used in social communication, or (3) symbolic or imaginative play.
- The disturbance is not better accounted for by Rett's Disorder or Childhood Disintegrative Disorder.
The Diagnostic and Statistical Manual's diagnostic criteria in general is controversial for being vague and subjective. (See the DSM cautionary statement.) The criteria for autism is much more controversial and some clinicians today may ignore it completely, instead solely relying on other methods for determining the diagnosis.
Epidemiology of autism[]
The Centers for Disease and Control and Prevention (CDC) states that:
- About 1 in 68 children has been identified with autism spectrum disorder (ASD) according to estimates from CDC’s Autism and Developmental Disabilities Monitoring (ADDM) Network.
- ASD is reported to occur in all racial, ethnic, and socioeconomic groups.
- ASD is about 4.5 times more common among boys (1 in 42) than among girls (1 in 189).
- Studies in Asia, Europe, and North America have identified individuals with ASD with an average prevalence of between 1% and 2%.
- About 1 in 6 children in the United States had a developmental disability in 2006-2008, ranging from mild disabilities such as speech and language impairments to serious developmental disabilities, such as intellectual disabilities, cerebral palsy, and autism.
Increase in diagnoses of autism[]
- For more details on this topic, see Frequency of autism.
{kind=link}
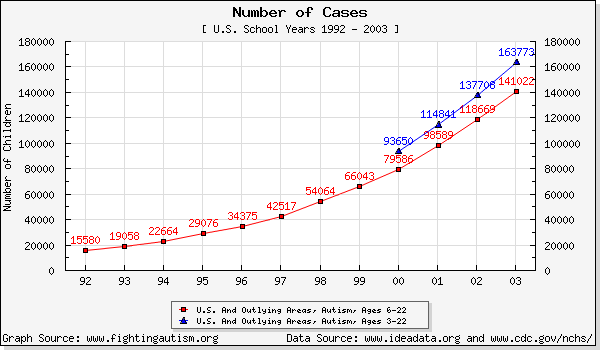
The number of reported cases of autism has increased dramatically over the past decade. Statistics in graph from the National Center for Health Statistics.
Autism has been diagnosed much more over the last ten years, similar to increases in the diagnosis of schizophrenia and multiple personality disorder in the twentieth century. This has brought rise to a number of different theories as to the nature of the sudden increase.
Common theories include:
- Autism rates are constant. The reported rise is due to better recognition of autistic people.
- Intelligent parents are more likely to have autistic children.[21] If more intelligent people produce offspring together, then more autistic children would be born.
- Some environmental factor (e.g. pollution, diet, or societal changes) is making more fetuses autistic.
- Autism is being over-diagnosed. People who would have been labeled as quirky or gifted are now receiving autism diagnoses. See clinomorphism for further discussion of this issue.
Epidemiologists argue that the rise in diagnoses in the United States is partly or entirely attributable to changes in diagnostic criteria, reclassifications, public awareness, and the incentive to receive federally mandated services. A widely cited study from the M.I.N.D. Institute in California (17 October 2002), claimed that the increase in autism is real, even after those complicating factors are accounted for (see reference in this section below).
Other researchers remain unconvinced (see references below). Dr. Chris Johnson, a professor of pediatrics at the University of Texas Health Sciences Center at San Antonio and cochair of the American Academy of Pediatrics Autism Expert Panel, said, "There is a chance we're seeing a true rise, but right now I don't think anybody can answer that question for sure." (Newsweek reference below).
The answer to this question has significant ramifications for the direction of research, since a real increase would focus more attention (and research funding) on the search for environmental factors, while little or no real increase would focus more attention to genetics.
As awareness of autism increases, an increasing number of adults with autistic traits seek diagnosis. As autism is mostly genetic, some of these adults are parents of autistic children who recognized autistic traits in themselves. Because autism falls into the pervasive developmental disorder category, strictly speaking, symptoms must have been present in a given patient before age seven in order to make a differential diagnosis.
Assessment of Autism[]
There are two broad approaches to autism assessments. One approach uses standardized tests and measures. The second approach relies more on clinical interviews, direct observations, and behavioral assessments.
Tests and Measures include the following:
- The Autism Diagnostic Interview-Revised [22]
- The Autism Diagnostic Observation Scale [23]
- Pre-Linguistic Autism Diagnostic Observational Schedule [24]
- Rimland's Diagnostic Checklist for Behavior-Disturbed Children, revised from E-2. [25]
Types of autism[]
Autism is a spectrum condition. While it was previously thought of as linear, experts now consider it multidimensional, with many different aspects.
Challenges to classifying autism subtypes[]
Autism is highly heterogenous. Some autistic people have high support needs and are incapable of independent living. Others are able to to live independently and work jobs with minimal support.
Many autistic people have "spiky skill profiles." This means that an individual could have severe impairments in some area while being near average or above average in others. For example, an autistic person who can carry on pleasant conversation skills and work full-time may also have profound developmental delays and be unable to cook, drive, or manage money. A nonspeaking person who stims frequently may also be intelligent and talented.
DSM-IV categories[]
{kind=link}
Asperger described his patients as "little professors".
The DSM-IV used several different categories for types of autism. These types were merged into Autism Spectrum Disorder in the DSM-5.
"Asperger syndrome" was formerly used to describe autistic people who didn't show strong developmental or social delays before the age of 3.
Pervasive developmental disorder not otherwise specified, or PDD-NOS, is referred to as a subthreshold condition. This label was sometimes given to people who had significant autistic traits but might not fully match the criteria for autism. PDD-NOS has no specific guidelines for diagnosis, so the person may have a lot of characteristics of an autistic person, or few to none at all.
Proposed subtypes[]
Some people have suggested that "classical autism" includes regressive autism and early infantile autism. Some autistic children experience regression around the age of 18 months for unknown reasons, while others do not.
Autistic people were previously categorized as "high-functioning" or "low-functioning." Many autistic people and some researchers have argued that these labels are reductive and harmful. People labeled as "high-functioning" may have their needs ignored, while "low-functioning" people may have their skills and agency ignored. These stereotypes can cause great harms to the individual.
Autistic people have proposed the labels "high/medium/low support" as replacements. These describe needs without inviting assumptions about abilities.
DSM-V changes[]
In 2013, the new edition of the DSM has classified all autistic disorders into a single diagnosis called Autism Spectrum Disorder, removing Asperger's Syndrome, Childhood disintegrative disorder (CDD) and PDD-NOS altogether, and treating Rett Syndrome as a separate genetic disorder. People diagnosed with Asperger syndrome, CDD, and PDD-NOS have been diagnosed with autism.
Some people applauded the merging of autism into a single diagnoses. Others preferred their previous diagnoses, such as Asperger syndrome. However, the term Asperger syndrome quickly fell out of popularity when it came to light that he sent some autistic children to Nazi death camps.
Causes and etiology[]
- For more details on this topic, see Causes of autism.
Therapies[]
- For more details on this topic, see Autism therapies.
Sociology[]
Due to the complexity of autism, there are many facets of sociology that need to be considered when discussing it. Autistic people have developed their own culture, especially online. There is also a culture of parents and others who see autism as a terrible disease.
Community[]
- For more details on this topic, see Autistic community.
- For more details on this topic, see Autism rights movement.
There are numerous resources, available from many groups, for autistics. Due to the fact that many autistics find it easier to communicate online than in person, many of these resources are available online. In addition, sometimes successful autistic adults in a local community will help out children with autism, much in the way a master would help out an apprentice, for example.
2002 was declared Autism Awareness Year in the United Kingdom.
Culture[]
- For more details on this topic, see Autistic culture.


{kind=link}
Autistic culture as illustrated by an autistic artist
With improvements in autism recognition and the rise of the internet, an autistic culture has begun to develop. Similar to deaf culture, autistic culture is based in a belief that autism is a unique way of being and not a disorder to be cured. There are some commonalities which are specific to autism in general as a culture, not just "autistic culture".
Some autistic people fall in love and marry. They are more likely to marry other autistic or neurodivergent people. Multigenerational autistic families are not uncommon.
The autism rights movement is a key aspect of autistic culture. Many autistic advocates advocate against the abuse and mistreatment of autistic people. They argue that harmless forms of self-expression and self-soothing, such as special interests and non-destructive stimming, should be accepted instead of punished.
Autistic culture has some parallels to geek and nerd culture.
Autistic adults[]


{kind=link}
Temple Grandin, a successful autistic adult. Photograph courtesy Joshua Nathaniel Pritikin and William Lawrence Jarrold.
Some autistic adults are able to work successfully in mainstream jobs. Still, navigating workplace dynamics and social expectations can be challenging. Some autistic people find it easier to work remotely. Other autistics can work in supported situations under the supervision of managers who are trained to help people with disabilities. A nurturing environment at home, at school, and later in job training and at work, helps autistic people continue to learn and to develop throughout their lives.
The internet can be a lifeline for autistic people. It allows them to communicate in writing without needing to navigate facial expressions and body language. It also makes it easier to find other autistic people and people who share their interests.
In the United States, the public schools' responsibility for providing services ends when the autistic person is in their 20s, depending on each state. The family is then faced with the challenge of finding living arrangements and employment to match the particular needs of their adult child, as well as the programs and facilities that can provide support services to achieve these goals.
Savant skills[]
- Main article: autistic savant
Some autistic people have "savant skills," or extreme talents in an area of study.
Although there is a common association between savants and autism (an association created by the 1988 film Rain Man), most autistic people are not savants. Mental calculators and fast programming skills are the most common form. The famous example is Daniel Tammet, the subject of the documentary film The Brain Man [1] (Kim Peek, one of the inspirations for Dustin Hoffman's character in the film Rain Man, is not autistic). "Bright Splinters of the Mind" is a book that explores this issue further.
Controversies[]
- Main article: Controversies in autism
Debates on autism often split into two groups. The neurodiversity group argues that autism is a difference instead of a disease, and that support for autistic people should honor their individual needs and quirks. The anti-neurodiversity group argues that autism is a disease that should be cured or ameliorated through behavior training to make autistic people fit in.
The debate about curing autism continues as scientists learn more about causation. Pro-cure advocates, many of which are parents, argue that autism is a disease that causes suffering and should be erased. Anti-cure advocates, many of which are autistic adults, raise concerns about eugenics, loss of human diversity, and the ethics of potential selective abortion. They argue that autistic people are members of a minority group rather that deserves accommodation instead of eradication. Websites such as autistics.org present the view of the anti-cure group.
Another controversy is applied behavior analysis (ABA). Proponents argue that ABA greatly changes behavior and is beneficial for improving life skills. Critics raise concerns about ethical issues, risk of PTSD and psychological harm, and potential harms of training autistic people to mask.[26][27][28] Research on potential harms is minimal.
Other pervasive developmental disorders[]
Autism is one of several pervasive developmental disorders. Others are Rett syndrome, Childhood disintegrative disorder. Some of these are related to autism, while some of them are entirely separate conditions.
Rett syndrome[]
Rett syndrome is relatively rare, affecting one out of 10,000 to 15,000, almost exclusively females. After a period of normal development, autism-like symptoms begin to appear at sometime between 6 and 18 months of age. The child's mental and social development regresses; she no longer responds to her parents and pulls away from any social contact. If she has been talking, she stops; she cannot control her feet; she wrings her hands. Some of these early symptoms may be confused with autism. Some of the problems associated with Rett syndrome can be treated. Physical, occupational, and speech therapy can help with problems of coordination, movement, and speech.
Scientists sponsored by the National Institute of Child Health and Human Development have discovered that a mutation in the sequence of a single gene causes Rett syndrome, and can physically test for it with an 80% accuracy rate [2].
Rett syndrome in the past was sometimes classified as an autistic spectrum disorder, however most scientists agree that Rett syndrome is a separate developmental disorder and not part of the autistic spectrum [3].
Childhood disintegrative disorder[]
Childhood disintegrative disorder (CDD, and sometimes abbreviated as CHDD also) is a condition appearing in 3- or 4-year-old children who have developed normally until around age 2. Over several months, the child will deteriorate in intellectual, social, and language functioning from previously normal behaviour. This long period of normal development before regression helps differentiate CDD from Rett syndrome (and in fact it must be differentiated from autism in testing). The cause for CDD is unknown (thus it may be a spectrum disorder) but current evidence suggests it has something to do with the central nervous system [4] [5].
Further Reading[]
- General
- Groups
- Controversy
- Lists
- Theories
See also[]
- ADHD
- Asperger syndrome
- Autism rights movement
- Autistic children
- Developmental disabilities
- Disability rights movement
- Early infantile autism
- Eccentricity
- Hikikomori
- Neurodivergent masking
- Rett syndrome
- Schizoid personality disorder
- Schizophrenia
- Social anxiety disorder
- Stimming
- Theory of mind
References[]
- (2001). Rett syndrome (NIH Publication No. 01-4960). Rett syndrome. Rockville, MD: National Institute of Child Health and Human Development. URL accessed on July 30, 2005.
- Frombonne E. (2002). Prevalence of childhood disintegrative disorder. Autism 6 (2): 149-157.
- Volkmar RM and Rutter M. (1995). Childhood disintegrative disorder: Results of the DSM-IV autism field trial. Journal of the American Academy of Child and Adolescent Psychiatry 34: 1092-1095.
- REDIRECT Template:cite news
- PANDAS (Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococci) and PITAND (Paediatric Infection-triggered Autoimmune Neuropsychiatric Disorders). PANDAS & PITAND Syndromes. URL accessed on July 30, 2005.
- Closer to Truth: PBS, with Paul Ewald. Microbes -- Friend or Foe?. URL accessed on July 30, 2005.
- M.I.N.D. Institute Study Confirms Autism Increase. U.C. Davis. URL accessed on March 6, 2005.
- redirect template:cite news
- redirect template:cite news
- Wing L, Potter D. (2002). The epidemiology of autistic spectrum disorders: is the prevalence rising?. Mental Retardation and Developmental Disabilities Research Reviews 8 (3): 151–61. (abstract)
- Croen LA, Grether JK, Hoogstrate J, Selvin S. (2002 Jun). The changing prevalence of autism in California. Journal of Autism and Developmental Disorders 32 (3): 207-15. (abstract)
- Manev R, Manev H. Aminoglycoside antibiotics and autism: a speculative hypothesis. BMC Psychiatry. 2001;1:5. Epub 2001 10 October.[6]
Strock, Margaret (2004). Autism Spectrum Disorders (Pervasive Developmental Disorders). NIH Publication No. NIH-04-5511, National Institute of Mental Health, National Institutes of Health, U.S. Department of Health and Human Services, Bethesda, MD, 40 pp. http://www.nimh.nih.gov/publicat/autism.cfm
- Frith, U. (2003). Autism: Explaining the enigma. Cambridge: Cambridge University Press.
Further reading[]
- The Autism Encyclopedia (John T. Neisworth, Ph.D., & Pamela S. Wolfe, Ph.D., 2004)
- The Autism Sourcebook: Everything You Need to Know about Diagnosis, Treatment, Coping and Healing (Karen Siff Exhorn, 2005)
- Sicile-Kira, C. (2004). Autism Spectrum Disorders.
- Behavioral Intervention for Young Children with Autism: A Manual for Parents and Professionals (edited by Catherine Maurice, 1996)
- Beyond the Autism Diagnosis: A Professional’s Guide to Helping Families (Marion O’Brien, Ph.D., & Julie A. Daggett, Ph.D., 2006)
- Powers, M.D. (2000). Children with Autism
- Wiseman, N.D. (2006). Could it be Autism?: A Parent’s Guide to the First Signs and Next Steps
Further reading[]
Books[]
- Gammeltoft, L & Nordenhof, M.S. (2007). Autism, play and social interaction. Jessica Kingsley.London.
Footnotes[]
- ^ NIH Autism Overview 2005. URL accessed on February 5, 2006.
- ^ BehaveNet autism description. URL accessed on July 30, 2005.
- ^ BehaveNet aspergers description. URL accessed on July 30, 2005.
- ^
- REDIRECT Template:cite news
- ^ autistics.org: The REAL Voice of Autism (See above). URL accessed on December 11, 2005.
- ^ Guardian "Brain Man" article. URL accessed on July 30, 2005.
- ^ NIH Rett description. URL accessed on July 30, 2005.
- ^ Bright Tots Rett description. URL accessed on July 30, 2005.
- ^ Yale CDD description. URL accessed on July 30, 2005.
- ^ NIH CDD description. URL accessed on July 30, 2005.
- ^ PDD-NOS at Yale. URL accessed on August 22, 2005.
External links[]
- General
- WrongPlanet.net - The Community and Resource for Autism
- Autism-Spectrum-Disorder.com - Autism Spectrum Disorder
- wikiHow's autism articles, many of which are edited by autistic people
- EricDigests.org - 'Teaching Students with Autism', Glen Dunlap, Lise Fox, ERIC Digest (October, 1999)
- Autistic and Proud Describes new discoveries about autism, autistics speaking for themselves.
- Weird Not Stupid - A website created from the perspective of a person who has two siblings who are on the Autism Spectrum with the goal of giving information to anybody who is seeking it.
- Autism Wiki A wiki About autism written mainly by autistics and their loved ones which offers views on autism from an autistics point of view
- Blogs
- Autism/Pervasive Developmental Disorders By Adelle Jameson Tilton, About.com
- Autism News and More
- Adventures In Autism By a health professional who is the mother of an autistic boy.
- Autism Symptoms
- Autistic Dreams by Luna Rose, an autistic adult
- Reality ABA, An Autism Diary By Katherine Lee, mother of an autistic son.
- Organizations
- autismwebsite.com Autism Research Institute Clearinghouse for information relating to autism, particularly the biomedical treatment approach
- Autism-Society.org - Autism Society of America
- autistics.org - Clearinghouse for information related to autism, from a non-cure standpoint. Many articles by autistics.
- Center for the Study of Autism, Autism Research Institute (founded by Bernard Rimland)
- Resources
- A Way Of Life Resources and information for parents.
- Autism Treatment Info Treatment Tips for Children with Autism, PDD & Asperger's Syndrome.
- Autism-Resources.com - Offering information and links regarding the developmental disabilities autism and Asperger's Syndrome.
- Autism Talk Parents & educators discuss all views.
- AutismToday.com - 'everything you need to know about autism', Autism Today
- Focus on Autism Selection of documentaries, interviews, etc.
- Autism.org.uk - 'PARIS: Public Autism Resource & Information Service' (directory of UK autism services)
- Autism Spectrum Quotient - Measure Your Autism Spectrum Quotient
- Aspie-quiz - Quiz that measures autistic traits
Pervasive developmental disorders / Autism spectrum | |
|---|---|
| Main |
Causes • Comorbid conditions • Epidemiology • Heritability • Sociological and cultural aspects • Therapies |
| Diagnoses |
Asperger syndrome • Autism • Childhood disintegrative disorder • PDD-NOS |
| Related conditions |
Epilepsy • Fragile X syndrome • High-functioning autism • Hyperlexia • Rett syndrome |
| Controversies |
Autism rights movement • Autistic enterocolitis • Chelation • MMR vaccine • Neurodiversity |
| Lists |
Autism-related topics • Further reading on Asperger syndrome • |
| Groups |
Aspies For Freedom • Autism Network International • Autistic Self Advocacy Network |
| This page uses Creative Commons Licensed content from Wikipedia (view authors). |
- ↑ Taboas, A., Doepke, K., & Zimmerman, C. (2023). Preferences for identity-first versus person-first language in a US sample of autism stakeholders. Autism, 27(2), 565-570. https://doi.org/10.1177/13623613221130845
- ↑ Identity-First Language
- ↑ Conceptualising Autistic Masking, Camouflaging, and Neurotypical Privilege: Towards a Minority Group Model of Neurodiversity
- ↑ Cassidy S, Bradley L, Shaw R, Baron-Cohen S. Risk markers for suicidality in autistic adults. Mol Autism. 2018 Jul 31;9:42. doi: 10.1186/s13229-018-0226-4. PMID: 30083306; PMCID: PMC6069847.
- ↑ Cassidy, S.A., Gould, K., Townsend, E. et al. Is Camouflaging Autistic Traits Associated with Suicidal Thoughts and Behaviours? Expanding the Interpersonal Psychological Theory of Suicide in an Undergraduate Student Sample. J Autism Dev Disord 50, 3638–3648 (2020). https://doi.org/10.1007/s10803-019-04323-3 Download citation
- ↑ Cage E, Di Monaco J, Newell V. Experiences of Autism Acceptance and Mental Health in Autistic Adults. J Autism Dev Disord. 2018 Feb;48(2):473-484. doi: 10.1007/s10803-017-3342-7. PMID: 29071566; PMCID: PMC5807490.
- ↑ Chapman, Louise; Rose, Kieran; Hull, Laura; Mandy, William (2022-11-01). ""I want to fit in… but I don't want to change myself fundamentally": A qualitative exploration of the relationship between masking and mental health for autistic teenagers". Research in Autism Spectrum Disorders. 99: 102069. doi:10.1016/j.rasd.2022.102069. ISSN 1750-9467. S2CID 253495529.
- ↑ Cook, J. M., Crane, L., & Mandy, W. (2024). Dropping the mask: It takes two. Autism, 28(4), 831-842. https://doi.org/10.1177/13623613231183059
- ↑ Damian E.M. Milton DEM979@bham.ac.uk (2012) On the ontological status of autism: the ‘double empathy problem’, Disability & Society, 27:6, 883-887, DOI: 10.1080/09687599.2012.710008
- ↑ Outcomes of real-world social interaction for autistic adults paired with autistic compared to typically developing partners
- ↑ Edey R, Cook J, Brewer R, Johnson MH, Bird G, Press C. Interaction takes two: Typical adults exhibit mind-blindness towards those with autism spectrum disorder. J Abnorm Psychol. 2016 Oct;125(7):879-885. doi: 10.1037/abn0000199. Epub 2016 Sep 1. PMID: 27583766.
- ↑ Double Empathy: Why Autistic People Are Often Misunderstood
- ↑ Sasson, N., Faso, D., Nugent, J. et al. Neurotypical Peers are Less Willing to Interact with Those with Autism based on Thin Slice Judgments. Sci Rep 7, 40700 (2017). https://doi.org/10.1038/srep40700
- ↑ Autistic Adults May Be Erroneously Perceived as Deceptive and Lacking Credibility
- ↑ Sasson, N. J., & Morrison, K. E. (2019). First impressions of adults with autism improve with diagnostic disclosure and increased autism knowledge of peers. Autism, 23(1), 50-59. https://doi.org/10.1177/1362361317729526
- ↑ Kapp SK, Steward R, Crane L, Elliott D, Elphick C, Pellicano E, Russell G. 'People should be allowed to do what they like': Autistic adults' views and experiences of stimming. Autism. 2019 Oct;23(7):1782-1792. doi: 10.1177/1362361319829628. Epub 2019 Feb 28. PMID: 30818970; PMCID: PMC6728747.
- ↑ Rethinking repetitive behaviors in autism
- ↑ Stimming, therapeutic for autistic people, deserves acceptance
- ↑ Why Lining Up Toys is Good For Autistic Kids
- ↑ How Can You Accommodate Autistic Students in the Classroom?
- ↑ Gardner RM, Dalman C, Rai D, Lee BK, Karlsson H. The Association of Paternal IQ With Autism Spectrum Disorders and Its Comorbidities: A Population-Based Cohort Study. J Am Acad Child Adolesc Psychiatry. 2020 Mar;59(3):410-421. doi: 10.1016/j.jaac.2019.04.004. Epub 2019 Apr 23. PMID: 31026573.
- ↑ Lord, C., Rutter, M., & Le Couteur, A., (1994). Autism Diagnostic Interview-Revised. Journal of Autism and Developmental Disorders, 24, 659-686.
- ↑ Lord, C., et. al., (1989). Autism Diagnostic Observation Schedule. Journal of Autism and Developmental Disorders, 19, 185-212.
- ↑ DiLavore, P., Lord, C., & Rutter, M. (1995). The Pre-Linguistic Autism Diagnostic Observation Schedule. Journal of Autism and Developmental Disorders.
- ↑ Rimland, B., (1971). The differentiation of childhood psychoses. Journal of Autism and Childhood Schizophrenia, 1, 161-174
- ↑ “Recalling hidden harms”: autistic experiences of childhood applied behavioural analysis (ABA)
- ↑ Aileen Herlinda Sandoval-Norton, Gary Shkedy & Dalia Shkedy | Jacqueline Ann Rushby (Reviewing editor) (2019) How much compliance is too much compliance: Is long-term ABA therapy abuse?, Cogent Psychology, 6:1, DOI: 10.1080/23311908.2019.1641258
- ↑ Evidence of increased PTSD symptoms in autistics exposed to applied behavior analysis